|
| Parathyroid gland has been listed as one of the Natural sciences good articles under the good article criteria. If you can improve it further, please do so. If it no longer meets these criteria, you can reassess it. | |||||||||
| ||||||||||
|
| A
fact from this article appeared on Wikipedia's
Main Page in the "
Did you know?" column on
July 9, 2014. The text of the entry was: Did you know ... that the
parathyroids were first discovered in the
Indian rhinoceros in 1852 but not identified in humans until 1880? | |||||||||
| This It is of interest to the following WikiProjects: | ||||||||||||||
| ||||||||||||||


Section on evolution requires an update.
There is actually significant evidence to show that the tetrapod parathyroid gland is directly homologous to gills in teleost fish. Professor Anthony Graham at King's College London has done lots of work with this.
The bottom line is that we still actually possess gills - they are just buried deep in our neck. If I get chance I will write this up. JoeNorris3K —Preceding unsigned comment added by 80.5.5.203 ( talk) 01:50, 1 May 2011 (UTC)
Who discovered these glands?
- Yeah, good question. My professor of surgery taught us it was first discovered in a rhinoceros at the London Zoo, and subsequently identified in humans. Sounds like an urban legend... Please let us know when you find out. JFW | T@lk 19:44, 12 Jun 2005 (UTC)
Ivar Sandstrom, a swedish medical student, discovered the parathyroid glands in 1880. I'll add with reference. GetAgrippa 13:41, 4 September 2006 (UTC)
I added neural crest contribution to induction of parathyroid. GetAgrippa 13:02, 4 September 2006 (UTC)
This section needs just a mention to evodevo and present evolution there. The article states: "A study published in the Proceedings of the National Academy of Sciences linked a regulatory gene to the formation of both the parathyroid glands in terrestrial vertebrates and gills in fish. Furthermore, two genes involved in calcium ion regulation were identified to be active in both structures. Thus both structures are thought to be homologous; 2006 (UTC)
References needed for this article.
Please consider change.
Your first two external links on parathyroid site are very commercial with lots of good and lots of bad infromation mixed together, pointing to each other as if to confirm their own validity but created by the same person. ultimately they are a commercial venture designed to direct patients to the surgeon who has created these pages. These sites have been well maintianed to ensure that they stay at the top of the search engines but may not be entirely reputable. Perhaps other reference would be better.
The following is also a bit confusing:
A blood calcium 15-30 minutes after the biopsy can help determine if the disease is caused by a single abnormal gland or multiple glands.
A drop in serum calcium suggests a single source, and no drop suggests multiple glands. This, with a non-localizing Sestamibi scan would point toward a neck exploration, rather than a minimally invasive method aimed a single gland disease.
US guided FNA identifies parathyroid glands and distinguishes them from LN or Thyroid nodule but can not tell if gland is hyperfunctioning. If lesion in correct location is larger than normal and is parathyroid it will most likely be the culprit.
Most physicians use drop in PTH (rather than calcium) in the operating room, 5 and 10 minutes following excision of a parathyroid to confirm biochemical correction/cure and to exclude multiple gland disease.
nonlocalizing scans are more common in multiglandular disease but may not preclude minimally invasive appraoch and neck exploration can be done "minimally invasive" as well
Please email if you have any questions. Thank you. —Preceding unsigned comment added by Bkmitchell (talk • contribs) 02:37, 7 January 2008 (UTC)
Retrieved from " http://en.wikipedia.org/wiki/User_talk:GetAgrippa" please consider changes The principle of the procedure is that the Tc99m-sestamibi is absorbed retained at a greater rate in a hyperfunctioning parathyroid gland than in a normal parathyroid gland. This is dependent on several histologic features within the abnormal parathyroid gland itelf. Sestamibi imaging is correlated with the number and activity of the mitochondria within the parathyroid cells, such that oxyphil parathyroid adenomas have a very high avidity for sestamibi, while chief cell adenomas have some affinity but to a lesser degree, and clear cell parathyroid adenomas have almost no imaging quality at all with sestambi. Some researchers have also attempted to quantitate or characterize the imaging capabilities of parathyroid glands by the MDR gene expression. Approximately 60 percent of parathyroid adenomas may be imaged by sestamibi scanning. The natural distribution of etiologic causation for primary hyperparathyroidism is roughtly 80 85 % solitary adenomas, 12 % diffuse hyperplasia, 2 % multiple adenomas, and 1 % cancer. In patients with multiglandular or ectopic parathyroid disease, imaging is not as reliable. In addition, size limitation of the abnormal gland can limit the detection by radionuclide scanning. By using a gamma camera in nuclear medicine, the radiologist is able to determine if one of the four parathyroid glands is hyperfunctioning, if that is the cause of the hyperparathyroidism. Theoretically, the hyperfunctioning parathyroid gland will take upretain more of the Tc99m-sestamibi, and will show up 'brighter' than the other normal parathyroid glands on the gamma camera pictures, especially because of the internal biofeedback loop within the body with calcium inherently feeding back to calcium-receptors and inhibiting parathyroid hormone production within the normal parathyroid glands. Sometimes this determination is made 2 to four hours later when activity taken up by the thyroid and normal parathyroid glands fade away; the abnormal parathyroid gland retains its activity, while the radiopharmaceutical is eluted out of the normal thyroid gland. However, in patients with nodular goiter or functional tumors of the thyroid gland, increased retention of the sestamibi agent is possible and make parathyroid localization difficult or confusing.
By knowing which of the four parathyroid glands is hyperfunctioning, a surgeon is able to remove only the one parathyroid gland that is producing excessive amounts of parathyroid hormone and no longer under the biochemical control of the body, and leave the other 3 normal parathyroid glands in place. This operation is now termed a "minimally invasive parathyroidectomy", sometimes utilizing a radionuclear detection probe, and correlated with intra-operative parathyroid hormone level measurements. The remaining 3 glands are able to properly regulate serum calcium levels appropriately after the resolution of the hypercalcemia, as the calcium receptors lead to stimulation of parathyroid hormone secretion.
Retrieved from " http://en.wikipedia.org/wiki/Sestamibi_scan" bkmitchell —Preceding unsigned comment added by Bkmitchell (talk • contribs) 03:13, 7 January 2008 (UTC)
Why is nothing written about the role in the (cellular) immune system? — Preceding unsigned comment added by 80.101.80.116 ( talk) 06:13, 24 September 2011 (UTC)
Could some knowledgeable and literate person re-write this section? "Parathyroid surgery is usually performed when there is hyperparathyroidism this conditions cause many diseases related with calcium reabsorption, because the principal function of the parathyroid hormone is to regulate it. Parathyroid surgery could be performed as two different ways the first one is the complete parathyroidectomy and the second one is the auto transplantation of the removed parathyroid glands." Seems hard to understand. Kortoso ( talk) 20:03, 29 May 2013 (UTC)
This paragraph was found directly lifted off a journal article:
Sandström was not aware of Owen’s description, which had been published in a journal with a limited circulation. Sandstrom's report was not well received and the work remained barely noticed for several years. Sandstrom suffered from a hereditary mental illness and unfortunately took his own life aged only 37 years.
I have done my best to remove any close-paraphrasing, but please correct any other instances if found. -- LT910001 ( talk) 02:57, 6 March 2014 (UTC)
| GA toolbox |
|---|
| Reviewing |
- This review is transcluded from Talk:Parathyroid gland/GA1. The edit link for this section can be used to add comments to the review.
Reviewer: Cwmhiraeth ( talk · contribs) 09:47, 26 May 2014 (UTC)
- I propose to review this article and am about to start working through it in detail. Cwmhiraeth ( talk) 09:47, 26 May 2014 (UTC)
First reading
Resolved comments from Cwmhiraeth
|
|---|
|
Clinical significance, history and other animals
Resolved issues from Cwmhiraeth
|
|---|
|
- I think that the ultra-structure of the chief cells and oxyphil cells should be included. It is interesting to see what the mysterious oxyphil cells look like under the electron microscope. Snowman ( talk) 18:15, 4 June 2014 (UTC)
I took a look and was very happy with the quality of the article. If there are any specific medical questions ( Cwmhiraeth please ask me and I will see if I can answer. My only points are two that I will fix myself if this is acceptable. They do not really have to do with the GA review save possibly the first one.
Under the history section I am missing mention of how early thyroidectomy was risk-filled seeing as the surgeons did not know of the parathyroid glands and if these were inadvertently removed they patients would die. I will add from either:
- I have a number of images on my computer awaiting cropping and uploading, some of which would be excellent for this article. I will upload these images first.
- --
CFCF (
talk ·
contribs ·
email) 19:42, 5 June 2014 (UTC)
- P.S. Both the above articles are sources of public domain images which I will also upload in the coming days.
CFCF (
talk ·
contribs ·
email) 19:46, 5 June 2014 (UTC)
- Thank you for your input into the article. I look forward to concluding the review within a few days.
Cwmhiraeth (
talk) 05:47, 6 June 2014 (UTC)
- Me too. I've boxed the comments that I feel I have resolved; if they're not, please unbox them and let me know.--
LT910001 (
talk) 09:05, 6 June 2014 (UTC)
- Ping to
Cwmhiraeth. I feel I have addressed your concerns. Is there anything that still needs to be done? --
LT910001 (
talk) 22:52, 8 June 2014 (UTC)
- I am proposing to do a final check on all aspects of the article shortly. Have you settled which images are to be used? The formatting of the references is not very consistent and could be improved. Cwmhiraeth ( talk) 18:53, 9 June 2014 (UTC)
- Ping to
Cwmhiraeth. I feel I have addressed your concerns. Is there anything that still needs to be done? --
LT910001 (
talk) 22:52, 8 June 2014 (UTC)
- Me too. I've boxed the comments that I feel I have resolved; if they're not, please unbox them and let me know.--
LT910001 (
talk) 09:05, 6 June 2014 (UTC)
- P.S. Both the above articles are sources of public domain images which I will also upload in the coming days.
CFCF (
talk ·
contribs ·
email) 19:46, 5 June 2014 (UTC)
GA Criteria
- 1a The article is well written.

- 1b The article conforms with the MOS guidelines with regard to layout and style.
- 2a&b The article is well referenced and has inline citations for all contentious statements.
The formatting of the references lacks consistency. - 2c There is no original research as far as I can see.
- 3a&b The coverage is broad enough and the article does not include irrelevant material.
- 4 The article is neutral.
- 5 The article has been edited by the nominator and other users but there has been no edit warring.
- 6 The images are in the public domain or have suitable licenses.
- 7 The images are relevant to the topic and have suitable captions.
- Overall assessment -
- Thanks, sorry, I will get to this in the coming day or two. --
LT910001 (
talk) 11:17, 11 June 2014 (UTC)
- Right. I've tried to remove the most egregious inconsistencies from the citations.
Cwmhiraeth, citations formatted in wiki-stye are not exactly my forte, if you can point out one or two examples of what else needs doing I'll get to it. --
LT910001 (
talk) 02:56, 13 June 2014 (UTC)
- I made one more change and the referencing now looks better. Well done. Cwmhiraeth ( talk) 05:20, 13 June 2014 (UTC)
- Right. I've tried to remove the most egregious inconsistencies from the citations.
Cwmhiraeth, citations formatted in wiki-stye are not exactly my forte, if you can point out one or two examples of what else needs doing I'll get to it. --
LT910001 (
talk) 02:56, 13 June 2014 (UTC)
These images are available for use in the article.


I will not be adding them myself as I intend to take part in the GA review process, so if you wish to add them you can do so LT910001
- Don't hesitate to ask me if you want them cropped in any way.
-- CFCF ( talk · contribs · email) 07:49, 4 June 2014 (UTC)
- There is no reason why you could not edit the page and also take part in the GA review; however, sometimes it might be simpler not to work on the page. Nevertheless, it is sensible to form a consensus about images, if you are in doubt. Snowman ( talk) 18:07, 4 June 2014 (UTC)
- The diagramme showing hormones (image 2) is probably more suitable for the calcium metabolism page. It could be useful here also. Any more opinions? Snowman ( talk) 18:07, 4 June 2014 (UTC)
- The anatomical diagramme is quite good, and could augment the a high resolution version of File:Gray1177.png. Snowman ( talk) 18:07, 4 June 2014 (UTC)
- Re File:Gray1177.png; this images in the gallery has poor resolution; however the 1918 PD version in Gray's is available at a much better resolution and can be uploaded over the poor quality image. I have look at a high resolution of this image and it looks quite good to me. Snowman ( talk) 18:07, 4 June 2014 (UTC)

Additional image from Grant's atlas. CFCF ( talk · contribs · email) 10:12, 6 June 2014 (UTC)
- I quite like these images, particularly the Grant's anatomy one, as it shows the glands from another angle. The other images are quite informative, but I feel they will need to bit quite big to be readable. -- LT910001 ( talk) 10:22, 6 June 2014 (UTC)
- The one with red parathyroid glands and red arteries looks odd to me, because sometimes the red there is an artery and sometimes red is a parathyroid gland. In diagrammes red is traditionally for arteries.
Snowman (
talk) 13:45, 7 June 2014 (UTC)
- Grant's anatomy atlas it the base of several newer anatomies, including Moore's clinically oriented anatomy, one of the major go-to text-books of anatomy for medical students. The image is the only one with any indication of the actual anatomy of the glands (not just rough whereabouts), and is the only one that has them visible in any form of close-up. Do you suggest we forego it because the color isn't to your liking?
CFCF (
talk ·
contribs ·
email) 15:48, 7 June 2014 (UTC)
- Points of view on images are subjective and what one person likes another may not. I would not object to using the one with the red parathyroid glands in the article. Nevertheless, I saw an image recently (forget where) that had yellow parathyroid glands and I looked quite good. Snowman ( talk) 16:57, 7 June 2014 (UTC)
- Grant's anatomy atlas it the base of several newer anatomies, including Moore's clinically oriented anatomy, one of the major go-to text-books of anatomy for medical students. The image is the only one with any indication of the actual anatomy of the glands (not just rough whereabouts), and is the only one that has them visible in any form of close-up. Do you suggest we forego it because the color isn't to your liking?
CFCF (
talk ·
contribs ·
email) 15:48, 7 June 2014 (UTC)
- Here is a black and white image from Gray's 1918. File:Anatomyofhumanbo1918gray 1280.jpg. It has a better resolution than the similar image in the gallery. Any comments? Snowman ( talk) 16:57, 7 June 2014 (UTC)


- I agree that they are fairly subjective. I'm not a big fan of black and white pencilled images, because I do not feel they have enough contrast to be seen well on a computer screen. I'd be very interested if you could find the yellow image that you mention. -- LT910001 ( talk) 22:03, 7 June 2014 (UTC)
How about this edit - #4

-- CFCF ( talk · contribs · email) 09:58, 8 June 2014 (UTC)
I've done a near exhaustive search for images of the parathyroid glands that are more than arrows or colored fields. They are very hard to bcome by even in non-free sources (and the best I can find is this: [1] [2] [3] Going back through a large number of anatomies these are the two I can come up with:
-
 The position of the para-thyroid glands. (Zuckerkandl.) http://babel.hathitrust.org/cgi/pt?id=uc1.b3888165;view=image;seq=34;page=root;size=100;orient=0
The position of the para-thyroid glands. (Zuckerkandl.) http://babel.hathitrust.org/cgi/pt?id=uc1.b3888165;view=image;seq=34;page=root;size=100;orient=0 -
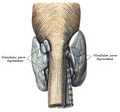 Glandulae parathyreoideae von hinten gesehen. http://babel.hathitrust.org/cgi/pt?id=uc1.b4100335;view=image;seq=222;page=root;size=100;orient=0
Glandulae parathyreoideae von hinten gesehen. http://babel.hathitrust.org/cgi/pt?id=uc1.b4100335;view=image;seq=222;page=root;size=100;orient=0 -
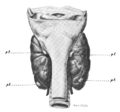 T. PARATHYROID GLANDIILES IN NORMAL SITUATION ON POSTERIORSURFACE OF THYROID GLAND. http://babel.hathitrust.org/cgi/pt?q1=parathyroid;id=mdp.39015077005620;view=image;seq=291;start=1;size=100;page=root;num=383;orient=0
T. PARATHYROID GLANDIILES IN NORMAL SITUATION ON POSTERIORSURFACE OF THYROID GLAND. http://babel.hathitrust.org/cgi/pt?q1=parathyroid;id=mdp.39015077005620;view=image;seq=291;start=1;size=100;page=root;num=383;orient=0



{kind=link}
![[1]](http://legacy.owensboro.kctcs.edu/gcaplan/anat2/notes/Image600.gif){kind=link}
![[2]](http://www.parathyroidglands.com/images/parathyroid-glands-2.jpg){kind=link}
![[3]](http://legacy.owensboro.kctcs.edu/gcaplan/anat2/notes/13_24.jpg){kind=link}
-- CFCF ( talk · contribs · email) 11:14, 8 June 2014 (UTC)
I quite like the "Glandulae parathyreoideae von hinten gesehen", I feel it's particularly clear, has some colour, and is not cluttered with the surrounding structures. I'd support including this but hope we can still retain the first lead image. I particularly like the current lead image because I think it is simple, modern, colourful, and conveys an idea about where the glands are and is, I feel, quite engaging to lay readers. -- LT910001 ( talk) 22:45, 8 June 2014 (UTC)
Variation
This will probably be the final image I add here, but this one is interesting as it gives some clue of variation:

This is a composite picture of all the glands found in 25 cadavers "plotted on a thyroid gland of average size and shape. The upper brackets indicate approximately the upper, middle and lower thirds of the thyroid; the lower bracket the space below the thyroid gland, the numbers giving the counts of the parathyroids within each bracket. The parathyroids are represented as if the thyroid were transparent. An attempt has been made to indicate the parathyroids which might be called 'superior parathyroids' in outline and 'inferior parathyroids' in black. Those glands which could not be classified either by location or by being one of a pair are cross- hatched" (Heinbach 1933).
-- CFCF ( talk · contribs · email) 10:19, 9 June 2014 (UTC)
- Wikipedia good articles
- Natural sciences good articles
- Wikipedia Did you know articles that are good articles
- GA-Class vital articles
- Wikipedia level-5 vital articles
- Wikipedia vital articles in Biology and health sciences
- GA-Class level-5 vital articles
- Wikipedia level-5 vital articles in Biology and health sciences
- GA-Class vital articles in Biology and health sciences
- GA-Class Anatomy articles
- High-importance Anatomy articles
- Anatomy articles about organs
- WikiProject Anatomy articles
|
| Parathyroid gland has been listed as one of the Natural sciences good articles under the good article criteria. If you can improve it further, please do so. If it no longer meets these criteria, you can reassess it. | |||||||||
| ||||||||||
|
| A
fact from this article appeared on Wikipedia's
Main Page in the "
Did you know?" column on
July 9, 2014. The text of the entry was: Did you know ... that the
parathyroids were first discovered in the
Indian rhinoceros in 1852 but not identified in humans until 1880? | |||||||||
| This It is of interest to the following WikiProjects: | ||||||||||||||
| ||||||||||||||
Section on evolution requires an update.
There is actually significant evidence to show that the tetrapod parathyroid gland is directly homologous to gills in teleost fish. Professor Anthony Graham at King's College London has done lots of work with this.
The bottom line is that we still actually possess gills - they are just buried deep in our neck. If I get chance I will write this up. JoeNorris3K —Preceding unsigned comment added by 80.5.5.203 ( talk) 01:50, 1 May 2011 (UTC)
Who discovered these glands?
- Yeah, good question. My professor of surgery taught us it was first discovered in a rhinoceros at the London Zoo, and subsequently identified in humans. Sounds like an urban legend... Please let us know when you find out. JFW | T@lk 19:44, 12 Jun 2005 (UTC)
Ivar Sandstrom, a swedish medical student, discovered the parathyroid glands in 1880. I'll add with reference. GetAgrippa 13:41, 4 September 2006 (UTC)
I added neural crest contribution to induction of parathyroid. GetAgrippa 13:02, 4 September 2006 (UTC)
This section needs just a mention to evodevo and present evolution there. The article states: "A study published in the Proceedings of the National Academy of Sciences linked a regulatory gene to the formation of both the parathyroid glands in terrestrial vertebrates and gills in fish. Furthermore, two genes involved in calcium ion regulation were identified to be active in both structures. Thus both structures are thought to be homologous; 2006 (UTC)
References needed for this article.
Please consider change.
Your first two external links on parathyroid site are very commercial with lots of good and lots of bad infromation mixed together, pointing to each other as if to confirm their own validity but created by the same person. ultimately they are a commercial venture designed to direct patients to the surgeon who has created these pages. These sites have been well maintianed to ensure that they stay at the top of the search engines but may not be entirely reputable. Perhaps other reference would be better.
The following is also a bit confusing:
A blood calcium 15-30 minutes after the biopsy can help determine if the disease is caused by a single abnormal gland or multiple glands.
A drop in serum calcium suggests a single source, and no drop suggests multiple glands. This, with a non-localizing Sestamibi scan would point toward a neck exploration, rather than a minimally invasive method aimed a single gland disease.
US guided FNA identifies parathyroid glands and distinguishes them from LN or Thyroid nodule but can not tell if gland is hyperfunctioning. If lesion in correct location is larger than normal and is parathyroid it will most likely be the culprit.
Most physicians use drop in PTH (rather than calcium) in the operating room, 5 and 10 minutes following excision of a parathyroid to confirm biochemical correction/cure and to exclude multiple gland disease.
nonlocalizing scans are more common in multiglandular disease but may not preclude minimally invasive appraoch and neck exploration can be done "minimally invasive" as well
Please email if you have any questions. Thank you. —Preceding unsigned comment added by Bkmitchell (talk • contribs) 02:37, 7 January 2008 (UTC)
Retrieved from " http://en.wikipedia.org/wiki/User_talk:GetAgrippa" please consider changes The principle of the procedure is that the Tc99m-sestamibi is absorbed retained at a greater rate in a hyperfunctioning parathyroid gland than in a normal parathyroid gland. This is dependent on several histologic features within the abnormal parathyroid gland itelf. Sestamibi imaging is correlated with the number and activity of the mitochondria within the parathyroid cells, such that oxyphil parathyroid adenomas have a very high avidity for sestamibi, while chief cell adenomas have some affinity but to a lesser degree, and clear cell parathyroid adenomas have almost no imaging quality at all with sestambi. Some researchers have also attempted to quantitate or characterize the imaging capabilities of parathyroid glands by the MDR gene expression. Approximately 60 percent of parathyroid adenomas may be imaged by sestamibi scanning. The natural distribution of etiologic causation for primary hyperparathyroidism is roughtly 80 85 % solitary adenomas, 12 % diffuse hyperplasia, 2 % multiple adenomas, and 1 % cancer. In patients with multiglandular or ectopic parathyroid disease, imaging is not as reliable. In addition, size limitation of the abnormal gland can limit the detection by radionuclide scanning. By using a gamma camera in nuclear medicine, the radiologist is able to determine if one of the four parathyroid glands is hyperfunctioning, if that is the cause of the hyperparathyroidism. Theoretically, the hyperfunctioning parathyroid gland will take upretain more of the Tc99m-sestamibi, and will show up 'brighter' than the other normal parathyroid glands on the gamma camera pictures, especially because of the internal biofeedback loop within the body with calcium inherently feeding back to calcium-receptors and inhibiting parathyroid hormone production within the normal parathyroid glands. Sometimes this determination is made 2 to four hours later when activity taken up by the thyroid and normal parathyroid glands fade away; the abnormal parathyroid gland retains its activity, while the radiopharmaceutical is eluted out of the normal thyroid gland. However, in patients with nodular goiter or functional tumors of the thyroid gland, increased retention of the sestamibi agent is possible and make parathyroid localization difficult or confusing.
By knowing which of the four parathyroid glands is hyperfunctioning, a surgeon is able to remove only the one parathyroid gland that is producing excessive amounts of parathyroid hormone and no longer under the biochemical control of the body, and leave the other 3 normal parathyroid glands in place. This operation is now termed a "minimally invasive parathyroidectomy", sometimes utilizing a radionuclear detection probe, and correlated with intra-operative parathyroid hormone level measurements. The remaining 3 glands are able to properly regulate serum calcium levels appropriately after the resolution of the hypercalcemia, as the calcium receptors lead to stimulation of parathyroid hormone secretion.
Retrieved from " http://en.wikipedia.org/wiki/Sestamibi_scan" bkmitchell —Preceding unsigned comment added by Bkmitchell (talk • contribs) 03:13, 7 January 2008 (UTC)
Why is nothing written about the role in the (cellular) immune system? — Preceding unsigned comment added by 80.101.80.116 ( talk) 06:13, 24 September 2011 (UTC)
Could some knowledgeable and literate person re-write this section? "Parathyroid surgery is usually performed when there is hyperparathyroidism this conditions cause many diseases related with calcium reabsorption, because the principal function of the parathyroid hormone is to regulate it. Parathyroid surgery could be performed as two different ways the first one is the complete parathyroidectomy and the second one is the auto transplantation of the removed parathyroid glands." Seems hard to understand. Kortoso ( talk) 20:03, 29 May 2013 (UTC)
This paragraph was found directly lifted off a journal article:
Sandström was not aware of Owen’s description, which had been published in a journal with a limited circulation. Sandstrom's report was not well received and the work remained barely noticed for several years. Sandstrom suffered from a hereditary mental illness and unfortunately took his own life aged only 37 years.
I have done my best to remove any close-paraphrasing, but please correct any other instances if found. -- LT910001 ( talk) 02:57, 6 March 2014 (UTC)
| GA toolbox |
|---|
| Reviewing |
- This review is transcluded from Talk:Parathyroid gland/GA1. The edit link for this section can be used to add comments to the review.
Reviewer: Cwmhiraeth ( talk · contribs) 09:47, 26 May 2014 (UTC)
- I propose to review this article and am about to start working through it in detail. Cwmhiraeth ( talk) 09:47, 26 May 2014 (UTC)
First reading
Resolved comments from Cwmhiraeth
|
|---|
|
Clinical significance, history and other animals
Resolved issues from Cwmhiraeth
|
|---|
|
- I think that the ultra-structure of the chief cells and oxyphil cells should be included. It is interesting to see what the mysterious oxyphil cells look like under the electron microscope. Snowman ( talk) 18:15, 4 June 2014 (UTC)
I took a look and was very happy with the quality of the article. If there are any specific medical questions ( Cwmhiraeth please ask me and I will see if I can answer. My only points are two that I will fix myself if this is acceptable. They do not really have to do with the GA review save possibly the first one.
Under the history section I am missing mention of how early thyroidectomy was risk-filled seeing as the surgeons did not know of the parathyroid glands and if these were inadvertently removed they patients would die. I will add from either:
- I have a number of images on my computer awaiting cropping and uploading, some of which would be excellent for this article. I will upload these images first.
- --
CFCF (
talk ·
contribs ·
email) 19:42, 5 June 2014 (UTC)
- P.S. Both the above articles are sources of public domain images which I will also upload in the coming days.
CFCF (
talk ·
contribs ·
email) 19:46, 5 June 2014 (UTC)
- Thank you for your input into the article. I look forward to concluding the review within a few days.
Cwmhiraeth (
talk) 05:47, 6 June 2014 (UTC)
- Me too. I've boxed the comments that I feel I have resolved; if they're not, please unbox them and let me know.--
LT910001 (
talk) 09:05, 6 June 2014 (UTC)
- Ping to
Cwmhiraeth. I feel I have addressed your concerns. Is there anything that still needs to be done? --
LT910001 (
talk) 22:52, 8 June 2014 (UTC)
- I am proposing to do a final check on all aspects of the article shortly. Have you settled which images are to be used? The formatting of the references is not very consistent and could be improved. Cwmhiraeth ( talk) 18:53, 9 June 2014 (UTC)
- Ping to
Cwmhiraeth. I feel I have addressed your concerns. Is there anything that still needs to be done? --
LT910001 (
talk) 22:52, 8 June 2014 (UTC)
- Me too. I've boxed the comments that I feel I have resolved; if they're not, please unbox them and let me know.--
LT910001 (
talk) 09:05, 6 June 2014 (UTC)
- P.S. Both the above articles are sources of public domain images which I will also upload in the coming days.
CFCF (
talk ·
contribs ·
email) 19:46, 5 June 2014 (UTC)
GA Criteria
- 1a The article is well written.
- 1b The article conforms with the MOS guidelines with regard to layout and style.
- 2a&b The article is well referenced and has inline citations for all contentious statements.
The formatting of the references lacks consistency. - 2c There is no original research as far as I can see.
- 3a&b The coverage is broad enough and the article does not include irrelevant material.
- 4 The article is neutral.
- 5 The article has been edited by the nominator and other users but there has been no edit warring.
- 6 The images are in the public domain or have suitable licenses.
- 7 The images are relevant to the topic and have suitable captions.
- Overall assessment -
- Thanks, sorry, I will get to this in the coming day or two. --
LT910001 (
talk) 11:17, 11 June 2014 (UTC)
- Right. I've tried to remove the most egregious inconsistencies from the citations.
Cwmhiraeth, citations formatted in wiki-stye are not exactly my forte, if you can point out one or two examples of what else needs doing I'll get to it. --
LT910001 (
talk) 02:56, 13 June 2014 (UTC)
- I made one more change and the referencing now looks better. Well done. Cwmhiraeth ( talk) 05:20, 13 June 2014 (UTC)
- Right. I've tried to remove the most egregious inconsistencies from the citations.
Cwmhiraeth, citations formatted in wiki-stye are not exactly my forte, if you can point out one or two examples of what else needs doing I'll get to it. --
LT910001 (
talk) 02:56, 13 June 2014 (UTC)
These images are available for use in the article.
I will not be adding them myself as I intend to take part in the GA review process, so if you wish to add them you can do so LT910001
- Don't hesitate to ask me if you want them cropped in any way.
-- CFCF ( talk · contribs · email) 07:49, 4 June 2014 (UTC)
- There is no reason why you could not edit the page and also take part in the GA review; however, sometimes it might be simpler not to work on the page. Nevertheless, it is sensible to form a consensus about images, if you are in doubt. Snowman ( talk) 18:07, 4 June 2014 (UTC)
- The diagramme showing hormones (image 2) is probably more suitable for the calcium metabolism page. It could be useful here also. Any more opinions? Snowman ( talk) 18:07, 4 June 2014 (UTC)
- The anatomical diagramme is quite good, and could augment the a high resolution version of File:Gray1177.png. Snowman ( talk) 18:07, 4 June 2014 (UTC)
- Re File:Gray1177.png; this images in the gallery has poor resolution; however the 1918 PD version in Gray's is available at a much better resolution and can be uploaded over the poor quality image. I have look at a high resolution of this image and it looks quite good to me. Snowman ( talk) 18:07, 4 June 2014 (UTC)
Additional image from Grant's atlas. CFCF ( talk · contribs · email) 10:12, 6 June 2014 (UTC)
- I quite like these images, particularly the Grant's anatomy one, as it shows the glands from another angle. The other images are quite informative, but I feel they will need to bit quite big to be readable. -- LT910001 ( talk) 10:22, 6 June 2014 (UTC)
- The one with red parathyroid glands and red arteries looks odd to me, because sometimes the red there is an artery and sometimes red is a parathyroid gland. In diagrammes red is traditionally for arteries.
Snowman (
talk) 13:45, 7 June 2014 (UTC)
- Grant's anatomy atlas it the base of several newer anatomies, including Moore's clinically oriented anatomy, one of the major go-to text-books of anatomy for medical students. The image is the only one with any indication of the actual anatomy of the glands (not just rough whereabouts), and is the only one that has them visible in any form of close-up. Do you suggest we forego it because the color isn't to your liking?
CFCF (
talk ·
contribs ·
email) 15:48, 7 June 2014 (UTC)
- Points of view on images are subjective and what one person likes another may not. I would not object to using the one with the red parathyroid glands in the article. Nevertheless, I saw an image recently (forget where) that had yellow parathyroid glands and I looked quite good. Snowman ( talk) 16:57, 7 June 2014 (UTC)
- Grant's anatomy atlas it the base of several newer anatomies, including Moore's clinically oriented anatomy, one of the major go-to text-books of anatomy for medical students. The image is the only one with any indication of the actual anatomy of the glands (not just rough whereabouts), and is the only one that has them visible in any form of close-up. Do you suggest we forego it because the color isn't to your liking?
CFCF (
talk ·
contribs ·
email) 15:48, 7 June 2014 (UTC)
- Here is a black and white image from Gray's 1918. File:Anatomyofhumanbo1918gray 1280.jpg. It has a better resolution than the similar image in the gallery. Any comments? Snowman ( talk) 16:57, 7 June 2014 (UTC)
- I agree that they are fairly subjective. I'm not a big fan of black and white pencilled images, because I do not feel they have enough contrast to be seen well on a computer screen. I'd be very interested if you could find the yellow image that you mention. -- LT910001 ( talk) 22:03, 7 June 2014 (UTC)
How about this edit - #4
-- CFCF ( talk · contribs · email) 09:58, 8 June 2014 (UTC)
I've done a near exhaustive search for images of the parathyroid glands that are more than arrows or colored fields. They are very hard to bcome by even in non-free sources (and the best I can find is this: [1] [2] [3] Going back through a large number of anatomies these are the two I can come up with:
-
The position of the para-thyroid glands. (Zuckerkandl.) http://babel.hathitrust.org/cgi/pt?id=uc1.b3888165;view=image;seq=34;page=root;size=100;orient=0
-
Glandulae parathyreoideae von hinten gesehen. http://babel.hathitrust.org/cgi/pt?id=uc1.b4100335;view=image;seq=222;page=root;size=100;orient=0
-
T. PARATHYROID GLANDIILES IN NORMAL SITUATION ON POSTERIORSURFACE OF THYROID GLAND. http://babel.hathitrust.org/cgi/pt?q1=parathyroid;id=mdp.39015077005620;view=image;seq=291;start=1;size=100;page=root;num=383;orient=0
-- CFCF ( talk · contribs · email) 11:14, 8 June 2014 (UTC)
I quite like the "Glandulae parathyreoideae von hinten gesehen", I feel it's particularly clear, has some colour, and is not cluttered with the surrounding structures. I'd support including this but hope we can still retain the first lead image. I particularly like the current lead image because I think it is simple, modern, colourful, and conveys an idea about where the glands are and is, I feel, quite engaging to lay readers. -- LT910001 ( talk) 22:45, 8 June 2014 (UTC)
Variation
This will probably be the final image I add here, but this one is interesting as it gives some clue of variation:
This is a composite picture of all the glands found in 25 cadavers "plotted on a thyroid gland of average size and shape. The upper brackets indicate approximately the upper, middle and lower thirds of the thyroid; the lower bracket the space below the thyroid gland, the numbers giving the counts of the parathyroids within each bracket. The parathyroids are represented as if the thyroid were transparent. An attempt has been made to indicate the parathyroids which might be called 'superior parathyroids' in outline and 'inferior parathyroids' in black. Those glands which could not be classified either by location or by being one of a pair are cross- hatched" (Heinbach 1933).
-- CFCF ( talk · contribs · email) 10:19, 9 June 2014 (UTC)
- Wikipedia good articles
- Natural sciences good articles
- Wikipedia Did you know articles that are good articles
- GA-Class vital articles
- Wikipedia level-5 vital articles
- Wikipedia vital articles in Biology and health sciences
- GA-Class level-5 vital articles
- Wikipedia level-5 vital articles in Biology and health sciences
- GA-Class vital articles in Biology and health sciences
- GA-Class Anatomy articles
- High-importance Anatomy articles
- Anatomy articles about organs
- WikiProject Anatomy articles