| This is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 | Archive 2 | Archive 3 | Archive 4 | Archive 5 |
Disruptive Activity
![]() Please stop your
disruptive editing. If you continue to
vandalize Wikipedia, as you did at
Paracetamol, you may be
blocked from editing. --
CFCF
🍌 (
email)
04:10, 27 July 2015 (UTC)
Please stop your
disruptive editing. If you continue to
vandalize Wikipedia, as you did at
Paracetamol, you may be
blocked from editing. --
CFCF
🍌 (
email)
04:10, 27 July 2015 (UTC)
- Yeah, so I add two interesting and important new, relevant references to an article which indicates potential harm to pregnant women on the Paracetamol page. These are removed because you guys don't like primary sources? This is ridiculous and frankly an extreme case of what is wrong with Wikipedia. My wife is pregnant. I for sure want to know about potential harm of this drug. I would think as a medical professional that you would be more inspired by the "first do no harm" idea. The fact that you Wikipedia jerks are so focused on having only sources from a narrow range of whatever it takes for a given article is so frustrating. I've continued to run into this kind of thing. You would think that academic journals have taken over Wikipedia. The idea that I have actually improved the article with my additions, and that others can improve it further, has completely escaped much of the Wikipedia culture these days. Wikipedia has simply forgotten the idea that this is collaboratively edited, rather than having a coterie of people who simply reject all edits if they do not thread the eye of the needle through the dozens of acronym style guides. You guys are disgusting, really. You are standing on the shoulders of millions of edits and now you reject the very thing that got you to where you are, namely lots of collaboratively edited small improvements. Now any change has to go through hurdles that would never have created Wikipedia in the first place. The fact that you have excluded something that is evidence of significant danger to pregnant women based on this culture of exclusiveness should trouble you deeply. -- Jeffmcneill ( talk) 06:21, 27 July 2015 (UTC)
- Jeffmcneill I'm sorry that I've upset you, but the fact is we get hundreds upon hundreds of poor quality changes every day. That is why we've written WP:MEDRS which I pointed to when I reverted you. There is also an excellent essay on why we adhere so strongly to it at WP:WHYMEDRS. The fact is that many primary studies are either performed on mice or on very small populations so that their results can't be transferred into clinical practise. MEDRS is no catch all, but it helps us and makes patrolling many articles and removing citations from the daily mail easier. I would also like to point out that we are working on getting these types of warnings into our articles automatically, for example by having FDA warnings automatically added.
- These were both large studies not having anything to do with mice. These rules are not useful, and essay reading should not be a requirement for submitting actual value to the article. Again, how would Wikipedia even exist if this kind of hurdle was required to get it started? This behavior is not sustainable. Eventually the remaining admins will actually reach the end of their productive lives and then what, Wikipedia will live on as a set of revert bots? Most likely. -- Jeffmcneill ( talk) 11:54, 27 July 2015 (UTC)
- I understand it may feel as if you're being reverted by a faceless mass, but I assure you if you had simply taken up the discussion it would have been far more likely to be productive. -- CFCF 🍌 ( email) 11:10, 27 July 2015 (UTC)
- This isn't about my feelings, it is about your behavior. You revert me with no reason, then start quoting this bureaucratic nonsense, then threaten me with banning due to my disruptive editing. This is why Wikipedia is dying, cannibalizing its editors and edits in a Kafkaesque farce. Congratulations, I'm sure your no-doubt proper and uplifting ZYZZYXRD will be cited upon its demise. You may want to try and comprehend your own actions, and not my feelings. See < http://www-users.cs.umn.edu/~halfak/publications/The_Rise_and_Decline/>. -- Jeffmcneill ( talk) 11:49, 27 July 2015 (UTC)
Asthma
There certainly seems to be an epidemiological association here, but I don't think consensus view is favors causation to the extent of the language that was added.
Here are the papers I found:
1) http://www.ncbi.nlm.nih.gov/pubmed/20933592: " At present, the evidence is inconclusive that any such association is causal."
2) http://www.ncbi.nlm.nih.gov/pubmed/23547988 " Is acetaminophen a real asthma promoter or an innocent bystander?"
3) http://www.ncbi.nlm.nih.gov/pubmed/23347656 "However, the epidemiological evidence is now compelling and there is a clear need to establish causation so that appropriate advice and interventions can be developed for children at risk of asthma. This requires randomised trials"
4) http://www.ncbi.nlm.nih.gov/pubmed/23292157 "Truly indicated antibiotics should not be withheld from infants or young children for fears they might develop asthma. Likewise, there is no sound reason to replace paracetamol as the preferred pain relief and fever medication in this age group."
5) http://www.ncbi.nlm.nih.gov/pubmed/23253685: "Causality cannot be established from observational studies because of the arguable presence of many confounding factors and biases. Randomised trials are needed to disclose the nature of the association"
6) http://www.ncbi.nlm.nih.gov/pubmed/21505328 "Several studies have shown an association between acetaminophen use during pregnancy and allergic diseases in the offspring. Furthermore, this association has also been found between early exposure and recent exposure to the drug and several allergic conditions. However, other studies did not confirm those associations."
Extensively quoting from what appears to be the single review of this area that unambiguously concludes a causative relationship is undue weight. Furhtermore, offering treatment guidance to avoid the use of acetominophen goes well outside published treatment guidelines and regulatory actions. NPOV requires that space alloted to different opinions should reflect their acceptance among experts. The modified language of this section does not do that. Formerly 98 ( talk) 05:03, 20 February 2014 (UTC)
- The epidemiological association between paracetamol and asthma is well established. The numerous factors indicating this association detailed and properly cited. Sources all peer reviewed medical journal articles.
- Concerned that this properly cited information from multiple credible sources has been repeatedly edited/deleted
- Sources: [1] [2] [3] [4]
- ^ McBride, J. T. (2011). "The association of acetaminophen and asthma prevalence and severity". Pediatrics. 128 (6): 1181–5. doi: 10.1542/peds.2011-1106. PMID 22065272.
- ^ Eneli, I; Sadri, K; Camargo Jr, C; Barr, R. G. (2005). "Acetaminophen and the risk of asthma: The epidemiologic and pathophysiologic evidence". CHEST Journal. 127 (2): 604–12. doi: 10.1378/chest.127.2.604. PMID 15706003.
- ^ Beasley, R; Clayton, T; Crane, J; von Mutius, E; Lai, C. K.; Montefort, S; Stewart, A; ISAAC Phase Three Study Group (2008). "Association between paracetamol use in infancy and childhood, and risk of asthma, rhinoconjunctivitis, and eczema in children aged 6-7 years: Analysis from Phase Three of the ISAAC programme". The Lancet. 372 (9643): 1039–48. doi: 10.1016/S0140-6736(08)61445-2. PMID 18805332.
- ^ Farquhar, H; Stewart, A; Mitchell, E; Crane, J; Eyers, S; Weatherall, M; Beasley, R (2010). "The role of paracetamol in the pathogenesis of asthma". Clinical & Experimental Allergy. 40 (1): 32–41. doi: 10.1111/j.1365-2222.2009.03378.x. PMID 20205695.
- Epidemiological associations do not prove causation by themselves. This sort of evidence is very similar to that which for many years was cited as evidence that post menopausal hormone replacement therapy prevents heart attacks in women. The Women's health initiative trial showed that the reduced cardiovascular events were not due to HRT, which actually increases CV risk, but to differing baseline characteristics of women who do and don't use HRT. That's why I'm so forceful about differentiating epidemiological association from causation here.
- I've cited about half a dozen articles in which experts state that they do not consider causation proven, including a few that state it is unlikely. Among the studies you have cited, the author of the first considers causality essentially proven. The second states that there is a "possible link". The third states that "paracetamol might be a risk factor". The fourth states that it is a "putative risk factor".
- So from among the 10 references that the two of us have found on this subject, one considers it proven that paracetamol causes asthma, and 9 draw conclusions varying from "it is unlikely that paracetamol causes asthma" to "it is likely but unproven". I don't understand why you have chosen to quote so extensively from the single article that considers the relationship essentially proven, when this seems to me to clearly be a minority (10%) viewpoint.
- Nor have I deleted the reference to asthma. I've merely toned down the statements regarding causation to match what seems to me to be mainstream opinion.
- Could we adjust the language to some mid point between what I had and your most recent version? Thanks Formerly 98 ( talk) 09:40, 20 February 2014 (UTC)
Nowhere in my edit was it claimed epidemiological associations prove causation. Indicated epidemiological association between paracetamol use and asthma well established. Detailed factors which firmly establish epidemiological association. Cited multiple references to peer reviewed medical journals supporting strong epidemiological association between paracetamol use and asthma. Epidemiological evidence invaluable and used to establish link between cigarette smoking and lung cancer. Added link to Epidemiology wiki page. Additionally, I left in your edit regarding possible debate word for word. Please stop deleting my accurate and properly referenced content. — Preceding
unsigned comment added by
BoboMeowCat (
talk •
contribs)
11:01, 20 February 2014 (UTC)
- Yes lots of reviews that discuss. Maybe be useful in a "research" section at the bottom of the article. I have removed the copy and pasted content as it is a copyright violation. Have also summarized in general terms and removed the primary research. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 14:13, 20 February 2014 (UTC)
I have compromised and cooperated fully. Edits regarding possible debate and possible confounding by indication were left in place word for word. Additionally, I’ve added a statement which explicitly indicates epidemiological associations do not prove causation. I had already linked to Epidemiology Wiki page for clarity. Despite this, my accurate and properly sourced information regarding strong epidemiological link to asthma has been repeatedly deleted. Because of this repeated occurrence, I’ve become concerned that “compromise” is being misused to mean censorship of accurate and properly referenced information regarding paracetamol’s well established epidemiological link to asthma.
My text was never copied and pasted, as words were changed. Wording has now been extensively changed to remove any remote hint of copyright violation. I’m going to ask again that this accurate and properly referenced information not be deleted, as repeatedly doing so suggests censorship of accurate information regarding epidemiological link to asthma and possible conflict of interest editing. –BoboMeowCat
- Bob, I'll wait for JMH649 to comment, but from my POV the issue with your new edit is the same as the old one. There are 10 relevant citations regarding this association, of which more than half say the case for causality is weak, and all but one of the remainder explicitly state that it is unproved. But while giving a nod to the idea that "association does not prove causation", you go on to present a counterpoint that lists out a long line of reasoning supporting the idea that it is essentially proven. Only one of 10 references supports this POV. You follow that up with a recommendation to avoid paracetamol in children that does not appear in any of the other 9 references (one of which recommends exactly the opposite).
- Pasting into Word, I count 143 words describing the single paper that supports your POV, and 60 words describing the 9 papers that don't. This is pretty much the definition of WP:RSUW. Its not that what you've said isn't a correct description of what is said in a WP:MEDRS compliant source. Its that you give undue space to a minority point of view relative to the majority POV. And that's equally against the rules here. Formerly 98 ( talk) 22:32, 21 February 2014 (UTC)
I'd like to ask that you please stop pretending I'm asserting causality rather than sharing accurate information regarding a very well established epidemiological association between paracetamol and asthma (which I followed with a detailed explanation of what makes this association so well established). I cited many sources to support. Also, please note explicit statement in my edit which indicates epidemiological associations do not prove causation. At this point, I'm fully expecting JMH649 will support you, as you summoned him in the first place, and his edits were extremely similar to your edits. I'm concerned that there appears to be an effort to censor accurate and properly referenced information, suggesting conflict of interest editing. If it is felt that information from any of your above mentioned sources is relevant, I'd like to ask you to please add that information as a separate edit, and refrain from again deleting accurate and properly referenced content. -- BoboMeowCat ( talk) 23:04, 21 February 2014 (UTC)
- Bob, all I'm asking is that you look at the paragraph you wrote and ask yourself if the average reader isn't going to walk away saying "wow, with that detailed list of points on how strongly the evidence favoring causation is, who are those nuts who aren't yet convinced that paracetamol causes asthma?" You've given a detailed account of one side of the argument and noted only that some don't agree with it.
- In fact, if you look at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3651816/ this author has provided a point by point rebuttal of each of the points that you quote from the McBride article. I could add these, but then the whole section becomes a rambling digression. It seems best just to keep it short since it is an unsettled issue.
- It would also be very helpful if you would lay off the accusations and abide by WP:GF. One could just as easily accuse you of being an agent of the companies that manufacture ibuprofen, especially as the only subject you have engaged on in some 35 Wikipedia edits is the role of acetominophen in asthma. As you can see, these sorts of personal attacks don't lead anywhere.
- Jmh by the way is the founder of the Wikipedia Medicine Project and the most senior person addressing medical issues in the organization. I thought he would probably support my position (because I think I am right), but he has overruled me on a number of occasions. He's not so much an ally of mine as someone who has broad overall responsibility for the medical content of the encyclopedia. I asked him to mediate as we were not reaching agreement among ourselves.
Formerly 98 (
talk)
00:54, 22 February 2014 (UTC)
- We are to summarize. The ref you removed was newer. So thanks Formerly for restoring the better version IMO. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 01:43, 22 February 2014 (UTC)
- Jmh by the way is the founder of the Wikipedia Medicine Project and the most senior person addressing medical issues in the organization. I thought he would probably support my position (because I think I am right), but he has overruled me on a number of occasions. He's not so much an ally of mine as someone who has broad overall responsibility for the medical content of the encyclopedia. I asked him to mediate as we were not reaching agreement among ourselves.
Formerly 98 (
talk)
00:54, 22 February 2014 (UTC)
Formelly 98 and Doc James, I’d like you to ask yourselves why you (or anyone for that matter) would want to censor accurate information regarding paracetamol’s very strong, repeatedly demonstrated, epidemiological link to asthma? If accurate and properly referenced information (from 5 credible sources, 2 of which were reviews of many studies) makes people think, “wow, this very well may be a concern”, then it seems that accurate information should not be censored by Wikipedia. I have browsed multiple medication pages on Wikipedia and browsed multiple edits. It appears that conflict of interest edits, on medication pages in particular, are common on Wikipedia. Such edits repeatedly downplay potential health concerns of medications. These edits appear to be made, in large part, by individuals with known or likely ties to the pharmaceutical industry.
Please add any properly referenced additional information and/or properly referenced rebuttals, as a separate edit. Again, please refrain from deleting accurate and properly referenced content, because censorship of this accurate information regarding paracetamol's well established epidemiological link to asthma seems to undermine the credibility and utility of Wikipedia. -- BoboMeowCat ( talk) 02:56, 22 February 2014 (UTC)
- Non-medical professional here, just weighing in with a fresh set of eyes. Bobmeowcat's most recent version did give the impression that the causal link was fairly well established ("not proved; HOWEVER!") , and I would infer a "suggested" medical recommendation in a reputable encyclopedia to be based on reasonably established scientific opinion. Granted, this is Wikipedia, and only fools would treat it as reputable, but we should still strive for accuracy and balance, particularly on issues of medical advice.
- BoboMeowCat, I realize this was your first foray into editing a Wikipedia article, at least with a user account, and it can seem like people are ganging up when you're making a sincere effort to improve the article. However, editors of medical articles are particularly cautious about controversial information based on isolated medical studies, and your contribution is exactly that. If you haven't already, I'd really suggest you take a look at Wikipedia's guidance on reliable sources for medical topics, at Wikipedia:MEDRS, particularly the opening section (the rest of it you could skim or skip, or read for clarification on cretain points). Other topics tend to be less stringent, and outside of academia there generally aren't equivalents of literature/systematic reviews, so there is more leeway in introducing non-mainstream opinions.
- Hmm...as I was typing this, I see that you reverted the reversions again. With all due respect, until there is a resolution on this issue, the controversial information should be removed. Jmh649 was asked to provide outside guidance on the issue. The short version is non-controversial, and does address the unestablished possibilty of causation. More importantly, be aware of the three revert rule ( WP:3RR) from the article on WP:EDITWARRING:
Bob we are to write in easy to understandable text. What you have added is much less understandable than what was there before. We all agree that there is an association. Is there proven causation? No and we should all be able to agree on that. That requires an RCT. One has not yet been done. Thus the association is tentative as it could be due to confounders. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 04:25, 22 February 2014 (UTC)
- Agyle, if accurate properly referenced information leads people believe this is cause for concern, that simply shows the evidence is strong and compelling. You appear to be arguing this evidence needs to be censored because it is too compelling. Additionally, this is not based on isolated medical studies. My current edit includes 11 references from peer reviewed medical journals including multiple articles which review numerous studies.-- BoboMeowCat ( talk) 15:29, 23 February 2014 (UTC)
Jmh649, only including information which suggests link not valid, while disallowing information which strongly suggests link valid, does not reflect neutrality. It is not balanced. The references to 11 primary and secondary sources included to illustrate that my edit does not represent "undue weight" material and my edit not based on "isolated studies". Regardless, accurate and extensively well referenced content again deleted, and I've been threatened with banning, if I were to restore this content. Please note, I've left in place your edits regarding possible doubt word for word. I have never deleted any of your or Formely 98's content. It is becoming clear that only information regarding doubt of association well be maintained, while all evidence suggesting link valid will be deleted. -- BoboMeowCat ( talk) 18:18, 23 February 2014 (UTC)
- There is an association. Now we need an RCT to look at the question. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 20:48, 23 February 2014 (UTC)
- Jmh649, I have zero objection to the addition of a statement regarding lack of RCT. If such a statement were added, I would not delete (as I have deleted zero content thus far, while my content repeatedly deleted). However, it does seem some would suggest ethical concerns regarding RCT in human pediatric population. Given the varied and abundant evidence linking paracetamol to asthma, such a study may be more ethical in animal model initially. --
BoboMeowCat (
talk)
21:24, 23 February 2014 (UTC)
- Wow you have obviously made up your mind. Anyway Wikipedia will update its content when more evidence is out. Right now all we have is an "association".
- We do have this 2013 review "there is no sound reason to replace paracetamol as the preferred pain relief and fever medication in this age group." [2]
- I see no reliable source claiming that acetaminophen causes asthma. Because of course currently the evidence is too weak to say it does. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 21:37, 23 February 2014 (UTC)
- Jmh649, I have zero objection to the addition of a statement regarding lack of RCT. If such a statement were added, I would not delete (as I have deleted zero content thus far, while my content repeatedly deleted). However, it does seem some would suggest ethical concerns regarding RCT in human pediatric population. Given the varied and abundant evidence linking paracetamol to asthma, such a study may be more ethical in animal model initially. --
BoboMeowCat (
talk)
21:24, 23 February 2014 (UTC)
- I have only "made up my mind" that the 11 studies referenced exist and have indicated the findings detailed (yet these findings have been repeatedly deleted). Interestingly, those who objected to the inclusion of this accurate content seem to have "made up minds", in a sense, because in this very talk section, it has been repeatedly conveyed to me that the evidence is too compelling to include.
- Additionally, a comprehensive review of asthma in pediatric population concluded: "Until future studies document the safety of this drug, children with asthma or at risk for asthma should avoid the use of acetaminophen"
- http://pediatrics.aappublications.org/content/early/2011/11/04/peds.2011-1106.full.pdf
- With your recent edit, you indicated the link may be due to confounding by indication (ie due to medications or illness coinciding with paracetamol usage). Evidence presented for this POV weaker and less well referenced, yet maintained, while more thoroughly referenced information deleted. Lack of neutrality/balance in the paracetamol asthma section troubling. -- BoboMeowCat ( talk) 23:04, 23 February 2014 (UTC)
- Bob, in spite of our disagreements, I think everyone here has been fairly diplomatic and respectful to you. But you seem locked into the idea that anyone who disagrees with you is an agent of the Evil Empire, and openly make accusations of bad faith as your primary tautological tool. As you can see, these types of tactics are not very successful here.
- I'd urge you to try a different tack. The current approach is not likely to achieve your goals. Formerly 98 ( talk) 23:12, 23 February 2014 (UTC)
- Instead of accusing me of wearing a tin foil hat, why not respond to my concerns. Why was less well referenced content regarding possible confounding by indication maintained, while more thoroughly referenced content suggesting valid link deleted? This does not seem to represent balance/neutrality. -- BoboMeowCat ( talk) 23:36, 23 February 2014 (UTC)
Hey User:BoboMeowCat. It appears that this is how you wish the section to appear. One of things we pay mind to is WP:WEIGHT. Can you please justify giving this section, which concerns an association and not an actual risk, equal weight with the liver toxicity section, which is an actual risk? The kind of argument that would be compelling, would be bringing a recent review article on overall acetaminophen toxicity that gives this association as much or more weight as liver toxicity. Thanks. Jytdog ( talk) 00:30, 24 February 2014 (UTC)
- We could summarize this as "A 2013 review concluded that paracetamol is perfectly appropriation for use in children at risk for asthma while 2011 review recommended that this group should avoid its use until there is further evidence" Anyway have added. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 00:33, 24 February 2014 (UTC)
- "Perfectly safe" does not seem to represent a balanced or neutral point of view. Additionally, presenting the information with the dates in this manner seems potentially misleading. It could easily be misinterpreted as suggesting the 2013 paper involved research demonstrating paracetamol's safety, therefore resolving the concerns brought up in the 2011 review, while this is not the case. --
BoboMeowCat (
talk)
01:08, 24 February 2014 (UTC)
- Yes we did not say "Perfectly safe"
Doc James (
talk ·
contribs ·
email) (if I write on your page reply on mine)
01:23, 24 February 2014 (UTC)
- Noted. You wrote "perfectly appropriate", which also does not seem balanced or neutral. — Preceding
unsigned comment added by
BoboMeowCat (
talk •
contribs)
01:34, 24 February 2014 (UTC)
- Yes because most of the literature still agrees that acetaminophen is "perfectly appropriate" Thus this wording is perfectly appropriate. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 01:45, 24 February 2014 (UTC)
- Noted. You wrote "perfectly appropriate", which also does not seem balanced or neutral. — Preceding
unsigned comment added by
BoboMeowCat (
talk •
contribs)
01:34, 24 February 2014 (UTC)
- Yes we did not say "Perfectly safe"
Doc James (
talk ·
contribs ·
email) (if I write on your page reply on mine)
01:23, 24 February 2014 (UTC)
- Jytdog, The difference is the liver toxicity section doesn't include text saying this is an epidemiological association which does not prove causation. Anyway, to clarify, the lack of balance/neutrality I was referring to was within the asthma subsection. In that subsection, only information suggesting link to asthma invalid included (ie due to medications or illness coinciding with paracetamol usage) while all evidence suggesting it may be a true link deleted, despite the fact that this evidence was referenced by 11 solid sources, including primary and secondary research. The claim regarding potential confounding by indication less well referenced, yet maintained. Lack of balance/neutrality --
BoboMeowCat (
talk)
01:20, 24 February 2014 (UTC)
- Thanks for responding, but that is not actually a response to my question about weight. (it is a response to why you want the content you want) Would you please respond to the question about weight? if you don't understand the question, please ask me to clarify it, thanks Jytdog ( talk) 01:24, 24 February 2014 (UTC)
- "Perfectly safe" does not seem to represent a balanced or neutral point of view. Additionally, presenting the information with the dates in this manner seems potentially misleading. It could easily be misinterpreted as suggesting the 2013 paper involved research demonstrating paracetamol's safety, therefore resolving the concerns brought up in the 2011 review, while this is not the case. --
BoboMeowCat (
talk)
01:08, 24 February 2014 (UTC)
- The American Pediatric Association recommends acetominophen for treating fever in children as of the May 2013 update of its website for parents.
http://www.healthychildren.org/English/safety-prevention/at-home/medication-safety/Pages/Acetaminophen-for-Fever-and-Pain.aspx. So it still seems to me that giving equal weight to a paper that suggests avoiding it is a little much. Nonetheless, if we can put this to bed I am fine with the current language. Thanks to everyone who worked on this, and especially to DJ, who put in a lot of time to mediate.
Formerly 98 (
talk)
01:31, 24 February 2014 (UTC)
- Yes agree we might currently be giving too much weight to the 2011 paper. Do we have a statement from the AAP we could add? Doc James ( talk · contribs · email) (if I write on your page reply on mine) 01:48, 24 February 2014 (UTC)
- The American Pediatric Association recommends acetominophen for treating fever in children as of the May 2013 update of its website for parents.
http://www.healthychildren.org/English/safety-prevention/at-home/medication-safety/Pages/Acetaminophen-for-Fever-and-Pain.aspx. So it still seems to me that giving equal weight to a paper that suggests avoiding it is a little much. Nonetheless, if we can put this to bed I am fine with the current language. Thanks to everyone who worked on this, and especially to DJ, who put in a lot of time to mediate.
Formerly 98 (
talk)
01:31, 24 February 2014 (UTC)
- Nice find! I just took my shot at crafting some language. It seems pretty clear that expert opinion is divided because there is lack of sufficient data, and in my view, the best Wikipedia can do is clearly acknowledge that. Let me know what you all think. Formerly, I used the section from the APA on OTC medicine in general, as it makes it clear that they do not drive parents toward ibuprofen over acetaminophen. Jytdog ( talk) 01:56, 24 February 2014 (UTC)
Simplier
This sentence is a little long "As of 2014, because there is insufficient data to determine if paracetamol use by pregnant women and young children causes asthma, [1] and there are different approaches to risk management, expert opinion is divided as to whether paracetamol should continue to be administered to pregnant women and children as it has in the past, [2] [3] whether paracetamol administration should be limited to cases where there is no good substitute, such as in infants younger than 3 months, [4] or if its use should be avoided until its safety is proven. [5]" Could use some simplification. The AAP deems acetaminophen to be appropriate to use to help with confort in children. [3]. The community is not exactly divided. Those recommending acetaminophen not be used are definitely the smaller group. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 02:03, 24 February 2014 (UTC)
- Hey DocJames. What I hear you saying, is the most relevant "major medical or scientific body" (to cite MEDRS) has not changed its opinion, and that is the best source to determine what the mainstream view is. True? If so, that makes sense and makes it clear that we give 'no change' the greater weight. I changed it accordingly:
- "As of 2014, the recommendations for acetaminophen use have not changed [6] but some experts have recommended restricting or avoiding its use in children and pregnant women. [7] [8]" Jytdog ( talk) 02:31, 24 February 2014 (UTC)
-
^ Cite error: The named reference
Hendersonwas invoked but never defined (see the help page). -
^ Heintze, K (2013 Jun). "The case of drug causation of childhood asthma: antibiotics and paracetamol". European journal of clinical pharmacology. 69 (6): 1197–209.
PMID
23292157.
{{ cite journal}}: Check date values in:|date=( help); Unknown parameter|coauthors=ignored (|author=suggested) ( help) - ^ American Academy of Pediatrics Last Updated July 10, 2013 Common Over-the-Counter Medications Page accessed February 23, 2014
- ^ Martinez-Gimeno A, García-Marcos L. The association between acetaminophen and asthma: should its pediatric use be banned? Expert Rev Respir Med. 2013 Apr;7(2):113-22. PMID 23547988
-
^ McBride, JT (2011 Dec). "The association of acetaminophen and asthma prevalence and severity". Pediatrics. 128 (6): 1181–5.
PMID
22065272.
{{ cite journal}}: Check date values in:|date=( help) - ^ American Academy of Pediatrics Last Updated July 10, 2013 Common Over-the-Counter Medications Page accessed February 23, 2014
- ^ Martinez-Gimeno A, García-Marcos L. The association between acetaminophen and asthma: should its pediatric use be banned? Expert Rev Respir Med. 2013 Apr;7(2):113-22. PMID 23547988
-
^ McBride, JT (2011 Dec). "The association of acetaminophen and asthma prevalence and severity". Pediatrics. 128 (6): 1181–5.
PMID
22065272.
{{ cite journal}}: Check date values in:|date=( help)
- Might be good to look at the recommendations of whatever the European equivalent of the AAP is. Having put this much time into this, we might as well do everything possible to reach a definitive conclusion. Formerly 98 ( talk) 02:41, 24 February 2014 (UTC)
- dug up the most recent EMA statement, which I got off the UK NHS press release reacting to recent data, which I also linked to. Jytdog ( talk) 07:18, 24 February 2014 (UTC)
- OK, so hopefully this issue is laid to rest now.
Jytdog (
talk)
07:18, 24 February 2014 (UTC)
- Current text: "There is an association between paracetamol use and asthma but it is unclear if it has a role in causing asthma.[42] As of 2014, the recommendations for acetaminophen use have not changed[43][44][45][46][47]:6-7 but some experts have recommended not using it in children and pregnant women.[48][49]" What recommendations? Changed from what? "Using it in..." seems like odd phrasing; "using it to treat..." seems more natural, although it still conveys a sense of something being done to them by someone else, which makes some sense for children, but not adults in countries where it's generally used without medical supervision; could switch to "...recommend X should not use Y" or something. Also, any chance "some experts" could be give any kind of indication of whether this was a common or obscure view? Citation [49], to my understanding, suggested only that children with asthma or at risk of asthma should avoid use of paracetamol, and said nothing about children in general, or pregnant women. Citation [48] has a worthless abstract and I'm not paying $84 to rent the full text for 24 hours. :-) If someone would quote the relevent sentence or two from the conclusion I'd sure appreciate it, for example [49] says “Until future studies document the safety of this drug, children with asthma or at risk for asthma should avoid the use of acetaminophen.” –– Agyle ( talk) 12:11, 24 February 2014 (UTC)
- Thanks for this helpful feedback. Ref 49 is Mcbride, who takes the risk very seriously - in the body of the article he writes: "At present, however, I need further studies not to prove that acetaminophen is dangerous but, rather, to prove that it is safe. Until such evidence is forthcoming, I will recommend avoidance of acetaminophen by all children with asthma or those at risk for asthma and will work to make patients, parents, and primary care providers aware of the possibility that acetaminophen is detrimental to children with asthma. " Ref 48 is Martinez-Gimeno, which says:
Expert commentary
Too liberal use of acetaminophen in childhood should no longer be recommended. There is a good deal of evidence suggesting that acetaminophen exposure is associated to the development of wheezing disorders and may increase its clinical manifestations in those children who already suffer them. Although the possibility still exists that acetaminophen is actually an innocent bystander, limiting its use to clinical situations in which no other alternatives remain offers practicing pediatricians a great opportunity to decrease wheezing incidence and morbidity in childhood with this simple and low-cost measure. Meanwhile, regulatory agencies should do their part and seriously reconsider the safety profile of acetaminophen and promote new and more definitive clinical trials evaluating this limiting intervention.
Five-year view
Most probably, the use of acetaminophen is going to decrease in the next few years from today's liberal use to a more limited one, but only when no other alternatives exist. Absolute banning does not seem possible or even adequate in the near future due to the lack of alternatives in some situations (newborns and infants below three months of age, intravenous use and ibuprofen contraindications such as ibuprofen intolerance and ibuprofen-associated serious gastrointestinal adverse events). This sharp decrease in population exposure to acetaminophen is likely to produce a measurable decrease in wheezing disorders prevalence and morbidity in childhood. "
- I clarified the text as per your request. Jytdog ( talk) 13:14, 24 February 2014 (UTC)
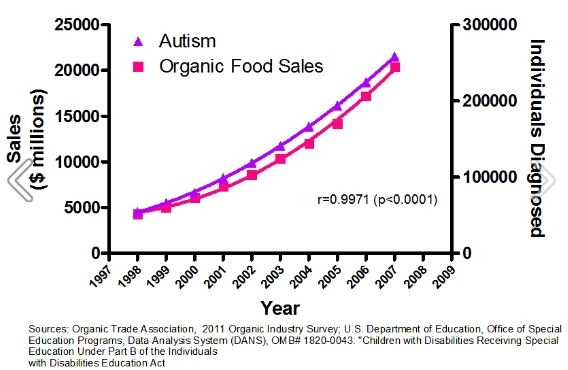
Nice work. Not to make light of a serious issue, but a very humorous take on correlation and causation here. Perhaps this image could be incorporated on the Monsanto page. http://www.pd.infn.it/~dorigo/autism_organic_foods.jpg Formerly 98 ( talk) 13:22, 24 February 2014 (UTC)
{kind=link}
- laughing! But seriously, Martinez-Gimeno bases their thoughts on the epidemiologial evidence and this study, which they describe as follows:
To test the hypothesis that acetaminophen exposure increases wheezing disorders severity or morbidity in asthmatic children, and its corollary, that avoiding acetaminophen exposure in asthmatic children would improve asthma control and morbidity, a more attainable clinical trial design would be needed, recruiting asthmatic children (several substudies with different age limits) to be randomized to one of two arms: intervention versus no intervention (open-labeled) or acetaminophen versus ibuprofen (double-blind design). Again, a placebo arm, contrary to common claims, would be impractical and unethical. Primary outcome could be one of the many already used: days free of symptoms, symptoms scores, drug consumption scores, asthma exacerbations or asthma-related quality of life, and the duration necessary to obtain enough statistical power would be in the range of months, not years.
In fact, such a clinical trial already exists [15] . It was performed in the early 1990s but published in the early 2000s, when the hypothesis of the detrimental effect of acetaminophen in asthma had already been launched. Being the only clinical trial ever performed on the subject, it deserves careful reading and a detailed description. From 2 February 1991 to 12 June 1993, 84,192 children between 6 months and 12 years of age with a febrile illness were recruited and randomly assigned to receive suspensions of either acetaminophen (12 mg/kg) or ibuprofen (5 or 10 mg/kg) to test the safety profile of ibuprofen. A subgroup analysis of those children being treated for asthma, defined as those who had received a [beta]-agonist, theophylline (remember, we were in the early 1990) or an inhaled steroid on the day before enrollment, identified an outstanding number of 1879 children, 632 randomized to acetaminophen, 636 to ibuprofen low-dose and 611 to ibuprofen high-dose. Primary outcomes were a report of hospitalization or outpatient visit for asthma in the month after enrollment. The number of hospitalizations was too low to reach significance (eight, four and six in the acetaminophen, low-dose ibuprofen and high-dose ibuprofen groups, respectively), but the number of outpatient visits for asthma was higher in the acetaminophen group compared with both ibuprofen groups (5.0 vs 2.9%). The authors reported this difference computing an adjusted relative risk estimate using the Mantel-Haenszel procedure; adjusting for age, gender and race and considering the acetaminophen group as the reference category: this estimate was 0.56 (0.34-0.95) for ibuprofen. This estimate did not vary when multiple stratifications where performed and did not differ between both ibuprofen doses. It should be taken into account that this clinical trial was originally designed to test the hypothesis that among children with asthma and without a history of aspirin sensitivity, ibuprofen suspension for fever-control increased the risk of acute bronchospasm and other morbidities from asthma. However, they found exactly the contrary. In their paper, the authors did not mention the reason for the 11 years elapsed between the end of the clinical trial and its publication. The possibility exists that their results were so unexpected and so contrary to common beliefs at the time that they only decided to publish them when the whole acetaminophen detrimental effect of wheezing disorders hypothesis begun to arise. Even to date, this large and well-designed clinical trial is not receiving due attention and some authors continue to explain their results as a beneficial effect of ibuprofen instead of a detrimental effect of acetaminophen. As practicing pediatricians, this discussion is absolutely irrelevant: avoiding acetaminophen is absolutely equivalent to using ibuprofen, because no other alternative exists.
- which is pretty interesting. Jytdog ( talk) 13:32, 24 February 2014 (UTC)
- Yes, its one of the more persuasive papers. But it also highlights the multiple hypothesis testing problem that is so common in the medical literature, and which can be so frustrating to deal with since publication in peer-reviewed journals gives the conclusions of these papers so much legitimacy. Since they included both previously asthmatic and non-asthmatic children in the study, I presume that they looked for the possibility of increased asthma in both subgroups as well as the overall treatment population. They looked at both hospitalization and non-hospitalization ER visits as endpoints. So I'm counting at least 5 shots at a p<0.05 outcome already, and I don't know if they would have published if they had seen differences at specific timepoints, changes in medication use, etc. I find articles like this in which the pre-specified endpoints of the trial are not disclosed very frustrating, because they are tantilizing, yet in the final analysis uninterpretable.
Formerly 98 (
talk)
14:06, 24 February 2014 (UTC)
- i hear you! Jytdog ( talk) 14:17, 24 February 2014 (UTC)
- Yes, its one of the more persuasive papers. But it also highlights the multiple hypothesis testing problem that is so common in the medical literature, and which can be so frustrating to deal with since publication in peer-reviewed journals gives the conclusions of these papers so much legitimacy. Since they included both previously asthmatic and non-asthmatic children in the study, I presume that they looked for the possibility of increased asthma in both subgroups as well as the overall treatment population. They looked at both hospitalization and non-hospitalization ER visits as endpoints. So I'm counting at least 5 shots at a p<0.05 outcome already, and I don't know if they would have published if they had seen differences at specific timepoints, changes in medication use, etc. I find articles like this in which the pre-specified endpoints of the trial are not disclosed very frustrating, because they are tantilizing, yet in the final analysis uninterpretable.
Formerly 98 (
talk)
14:06, 24 February 2014 (UTC)
One of our key roles here on Wikipedia is to take complicated verbiage and get to the point.
This "A 1998 paper hypothesized that giving young children paracetamol may cause asthma later in life and while subsequent epidemiological studies have found a correlation between paracetamol use by young children and pregnant women and asthma, as of February 2014 it remained unclear if paracetamol actually has a role in causing asthma."
really means
"There is an association between paracetamol use and asthma but it is unclear if it has a role in causing asthma."
with the latter being much more clear and to the point. Thus restored. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 18:10, 24 February 2014 (UTC)
- I hear you on that! The key reason why I added the 1998 paper was in response to the question from Agyle above, where he wrote "What recommendations? Changed from what?" I thought those were valid questions.
Jytdog (
talk)
18:27, 24 February 2014 (UTC)
- Added the recommendation. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 19:02, 24 February 2014 (UTC)
- I hear you on that! The key reason why I added the 1998 paper was in response to the question from Agyle above, where he wrote "What recommendations? Changed from what?" I thought those were valid questions.
Jytdog (
talk)
18:27, 24 February 2014 (UTC)
- /* Simplier */
talk, thanks for reponse & quotes from Martinez-Gimeno. Sentence seems clearer now. However, this part, "but some experts have recommended that paracetamol use by children and pregnant women should be avoided.[48][49]", raises these issues about agreement between the cited sources and that part of sentence.:
- Martinez-Gimeno/García-Marcos [ref 48] (from the excerpt I read) recommends stopping “too liberal use” and “limiting its use to clinical situations in which no other alternatives remain” for all children. This does not mention pregnant women (perhaps it's mentioned elsewhere in the article, in which case disregard this; certainly use by pregnant women is questionable for non-asthma reasons). Also it's not saying to avoid its use in children entirely, including an exception for clinical situations with no alternatives. Since there are two authors, "some experts" is technically correct.
- McBride [ref 49] recommends “children with asthma or at risk for asthma should avoid the use of acetaminophen.” (Emphasis mine.) He does not mention pregnant women, or include healthy children, in that recommendation. I think his is a distinctly different recommendation from the one described in the Wikipedia article, and should be omitted as a source, or his view presented in addition to Martinez-Gemino's.
- Hope I'm not coming off as too nitpicky; your synthesis of all this feedback seems very good. :-) –– Agyle ( talk) 23:56, 24 February 2014 (UTC)
- /* Simplier */
talk, thanks for reponse & quotes from Martinez-Gimeno. Sentence seems clearer now. However, this part, "but some experts have recommended that paracetamol use by children and pregnant women should be avoided.[48][49]", raises these issues about agreement between the cited sources and that part of sentence.:
- not too nit-picky at all and your questions are all about making the article great. the original 1998 hypothesis was about infants and young kids. but as folks thought about the hyopthesis and designed epidemiologial studies, some of them took it back yet further. McBride (source 49, which is free) talks about this just a bit in ~3rd paragraph of the intro (search for "utero"). i would not be at all opposed to deleting the pregnancy thing (especially since it is secondary for even the most worried guy, McBride) - but in light of bobo's fierce concern about this issue, and since it didn't take a lot of space and wasn't inaccurate, i included it. but i am fine with it being deleted too. Jytdog ( talk) 01:10, 25 February 2014 (UTC)
- I didn't address your concern about the variation in "avoidance". in one of my first stabs at this, i think i set up three paths - change nothing; Martinez (which we agree on - use it only where you gotta), and Mcbride, which i framed as "stop using it". but you are right - it is "don't use it in kids with asthma or at risk for asthma." and you are right that nobody says boo about changig what pregnant women do. i just took that out. struggling with the other, especially in light of simplier. :) hmmm ok, made it "paracetamol should be given to children more selectively" - that covers both mcbride and martinez, yes? Jytdog ( talk) 01:25, 25 February 2014 (UTC)
- Restored Doc James version: Given "more selectively" seems vague.
- If you feel strongly about including "more selectively", I would not object to it being included along with a statement that experts have suggested avoidance, but not in place of it. Seems unbalanced and a downplay of the expert opinions.-- BoboMeowCat ( talk) 01:54, 25 February 2014 (UTC)
- "feeling strongly" has nothing to do with it. at this stage it is about trying to set up language that is good enough so we can all move on. i do think that argyle had a legit point about pregnancy, so i am taking that back out but will leave the "avoid" - that is 6 of one half a dozen of the other to me. Jytdog ( talk) 02:04, 25 February 2014 (UTC)
- The current text omits antipyretic use as an acceptable use by children ("...continue to recommend paracetamol for pain and discomfort in children....") I'd say “pain and fevers”, or something to that effect. Perhaps include discomfort too; AAP gives aches and soreness as examples, and Sullivan 2011 mentions improving comfort with regard to antipyretics. The cited EMA/HMA source seems more conservative than American recommendations (contrast AAP's casual examples to EMA/HMA's ”paracetamol should only be used during pregnancy or in children if clearly necessary”), but I can see ignoring this in the interest of simplicity.
- Regarding BoboMeowCat's “unbalanced and a downplay of the expert opinions”, I was actually thinking exactly the opposite. References [43]-[45] were all written/updated after [48] (Martinez-Gimeno/García-Marcos), and presumably considered their recommendation. Based on its current rejection by the scientific establishment, I'd suggest changing "some experts" to "a few experts", to better reflect its weight compared to the mainstream position(s), unless the recommendation comes from more than a single (though admittedly very strong) source.
- Agyle,I understand the nature of your assumption, but rejection not supported by references. Recommendations may represent maintenance of the status quo.-- BoboMeowCat ( talk) 04:14, 25 February 2014 (UTC)
- The UK National Institute of Clinical excellence updated their recommendations for treatment of fever in children in May 2013 and recommended treatment with either ibuprofen or acetominophen, with no preference stated. http://publications.nice.org.uk/feverish-illness-in-children-cg160/recommendations.
- In 2012, the World Health Organization developed recommendations for the treatment of chronic pain in children, recommending that mild pain be treated with acetominophen or ibuprofen. http://www.ncbi.nlm.nih.gov/books/NBK138340/
- The Italian Pediatric Association updated their guidelines in 2012 and also recommended ibuprofen or acetominophen. http://www.ncbi.nlm.nih.gov/pubmed/22742886?dopt=Abstract&holding=f1000,f1000m,isrctn
- Formerly 98 ( talk) 05:17, 25 February 2014 (UTC)
- BoboMeowCat, good point, cited sources don't indicate that the AAP or NHS considered any published reviews, let alone Martinez-Gimeno. We're still left, however, with medical organizations and most several recent reviews on one side, and a two-author review on the other. (McBride falls in the middle, but his view & recommendation are omitted from the current Wikipedia text.) I only just got access to Martinez-Gimeno, and noticed that in its section on other experts' opinions ("Experts' Opinion & Attitudes to the Acetaminophen as a Wheezing Disorders Promoter Hypothesis"), it cites four recently published reviews with status quo opinions, which it attributes to bias, and only McBride's suggesting any change in paracetamol usage. While it may well be correct, Martinez-Gimeno's review itself seems to make a case that it's a minority view among experts. Agyle ( talk) 06:13, 25 February 2014 (UTC)
- The NHS meticulously documents its search and deliberation procedures, and these can be found for the acetominophen recommendation, including the exact details of the adverse event search in the following document. http://guidance.nice.org.uk/CG/WaveR/108/HEPlanReviewQuestionsSearchStrategies/ReviewQuestionsSearchStrategies/pdf/English. The search strategy explicitly includes Medline and other database searches for adverse event related publications. (page 183).
- In their 2011 Fever treatment guideline, the AAP explicitly mentions the asthma hypothesis and states: "One safety concern is the effect of acetaminophen on asthma-related symptoms; although asthma has also been associated with acetaminophen use, causality has not been demonstrated." Having noted this association in 2011, it strains credulity to think they would not have considered it when they updated the guideline in 2013. http://pediatrics.aappublications.org/content/127/3/580.full
- I reverted your edit because I think it takes us back to where we were at the beginning of this 8,000 word argument: by expanding on the language for the minority position, it not only gives equal weight to the minority position, it actually emphasizes it. I just don't think you can counterpoint the opinion of NICE and the AAP with the opinion of 3 or 4 researchers. Its not balanced. Formerly 98 ( talk) 10:15, 25 February 2014 (UTC)
- The amount of time and effort we have put into these two sentences is like something out of a Monty Python skit. I'd like to propose that we hold a simple vote, choosing between the most recent version by Argyle and the prior version by Jytdog, and then put this to bed. Having just reverted Argyle, I'm obviously casting my vote for the Jytdog version. Formerly 98 ( talk) 10:26, 25 February 2014 (UTC)
- Formerly 98, I think you're misunderstanding things. I didn't change either sentence whatsoever, and it is not “my version”. Four days ago I did revert Bobo's change, but other than that, have not changed the section's text in any way. The edit you reverted were merely changes within the citations themselves, mostly touchups like capitalizing journal names and adding links to the text of the articles, but also including two quotes from the conclusions of the studies within the citations. (If you object to that, then remove just the "quote=" parts in the citations, and we can discuss it further). I'm reverting your reversion, under the good faith belief that you misinterpreted my edit.
- Per the suggestion to "just put this to bed", which you also suggested earlier, in a word: no. If there are improvements to be made, they should be made. Saying it's ok for children for pain and discomfort, but omitting its use as an antipyretic, deviates from almost all of the cited sources. It's minor, but I'm not letting it slide just because you want to be done with this. Agyle ( talk) 11:01, 25 February 2014 (UTC)
- No, I did mean to revert. Having additional arguments that flash up when you roll the cursor over the text does increase the weight given to the "stop all acetominophen use in children" POV, which was already too high. We're taking two papers and counterpoising them against the opinion of expert panels at the American Academy of Pediatrics and a review at the National Institute of Clinical Excellence. I don't think it makes sense.
- You joined this discussion at a point after which I had already spent many hours of work on it, and so my fatigue may not be something you relate to. I've had to defend myself against an unwarranted COI investigation and endless insinuations that I was engaging in shilling for a corporate client as well. Its fine to disagree that the 7408 words that have been spent on the topic here and the additional words over at COIN are not sufficient. But "I'm not letting it slide just because you want to be done with it" seems unnecessarily dismissive and disrespectful. I've put a lot of work into this, and while I do not expect others to always agree with me, it would be nice if they showed some respect for my efforts. Your efforts to fine tune the language are built on a foundation of many hours of work that I put in getting us away from language that you yourself have criticized as giving readers an incorrect impression.
- To avoid any misunderstanding, the "Monty Python" remark was a gibe at the process overall, including my own 5000 or so word contribution to the aforementioned 7400 words. It was not intended as a criticism of your work, and I apologize if I failed to make that clear. Formerly 98 ( talk) 14:01, 25 February 2014 (UTC)
- Agyle and Formerly 98, while I see the point regarding the recommendations for current continuation of status quo being more numerous than recommendations for avoidance, it seems that inclusion of statement regarding avoidance seems appropriate, particularly in light of fact that the earlier statement regarding "unclear" appears unbalanced. While certainly not proven beyond all doubt, there is abundant and varied evidence, which would provide additional clarity on the issue, yet has already been deleted:
- https://www.ncbi.nlm.nih.gov/pubmed/22065272
- https://www.ncbi.nlm.nih.gov/pubmed/15706003
- https://www.ncbi.nlm.nih.gov/pubmed/18805332
- https://www.ncbi.nlm.nih.gov/pubmed/18201589
- https://www.ncbi.nlm.nih.gov/pubmed/20205695
- https://www.ncbi.nlm.nih.gov/pubmed/20709817
- https://www.ncbi.nlm.nih.gov/pubmed/15735054
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1745727/
- https://www.ncbi.nlm.nih.gov/pubmed/19210907
- https://www.ncbi.nlm.nih.gov/pubmed/19210907
- https://www.ncbi.nlm.nih.gov/pubmed/18400839
- Including all of this abundant and varied evidence would make the section considerably more lengthy, and in terms of briefly, the current statement regarding avoidance seems to provide some of the missing balance for all of the above mentioned omitted content.-- BoboMeowCat ( talk) 16:42, 25 February 2014 (UTC)
User:BoboMeowCat. The causal link is not proven; not a single source that you bring above says that it is. It is also a fact, as the article states, that the mainstream view has not yet shifted to changing acetaminophen administration to kids based on a concern about this. This is how wikipedia works; we give the WP:WEIGHT to the mainstream, consensus view, which we identify through the statements of major medical bodies, as we have done here. We represent, but give less weight to, minority views, which we have also done here. Wikipedia is not here to WP:RIGHTGREATWRONGS - we give the weight to the mainstream, consensus views. If you want to advocate for changing the mainstream view, Wikipedia is not the place to do it. Please read WP:ADVOCACY. When a mainstream medical body changes its recommendation based on a concern about asthma, we can revisit this. If you know of any that have done so, please bring a source for that. Until you do, the article is going as far as it can. I am giving you a heads up here now - I and others have explained, based on Wikipedia guidelines and policies, ( WP:MEDRS and WP:WEIGHT) how the content you are interested in is handled at Wikipedia. Further, no one is supporting your position that the mainstream says that acetaminophen causes asthma nor a position that the minority view deserves more weight. Please read WP:IDHT - you are getting pretty close to falling squarely within that. I for one am going to stop responding to you pretty soon, until you bring the kind of sources we need to go further. You are new here, so I am trying to warn you very clearly. If you continue to try to actually edit the article to increase the weight given to this issue, without bringing the kind of source needed to give it more weight, I'll bring you to the WP:NPOVN board, and you will get blocked again or perhaps even topic banned. I hope you do not go in that direction, but based on your behavior thus far (blocked for editing warring, then bringing a groundless COIN case, and coming back here and repeating yourself) my guess is that you are are not going to listen. I hope you do listen. best regards Jytdog ( talk) 18:06, 25 February 2014 (UTC)
- There seems to be misrepresentations present in the above comment. If you review my edits and talk history, it shows I've never stated it was proven that paracetamol causes asthma. I have not advocated policy change. However, I have objected to the repeated deletion of accurate and properly sourced content (which at this time remains deleted) because that seems unbalanced/not neutral. Specifically, this content includes factors which provide clarity regarding the epidemiological link to asthma. As this discussion has become very lengthy, I'll repeat factors:
- (1) a dose-response relationship between paracetamol use and asthma;
- (2) the results of a double blind trial comparing paracetamol to ibuprofen for treatment of fever in asthmatic children;
- (3) the strength of the association between paracetamol use and asthma;
- (4) the consistency of this association across different geographical areas and different cultures;
- (5) the timing of increased paracetamol use in relation to the asthma epidemic
- (6) a relationship between per-capita sales of paracetamol and asthma prevalence across multiple countries;
- (7) the association between use of paracetamol by mother during pregnancy and increased wheezing in early childhood; and
- (8) a biologically plausible mechanism of glutathione depletion in airway mucosa.
- These factors were referenced by the above linked 11 peer reviewed medical journal articles (which included both primary and secondary sources) yet it was deleted. Also please note, I have not reinstated this deleted content, but rather objected to the deletion of additional content, because that additional deletion, on top of the already significant deletion, would seem to further reduce balance/neutrality.-- BoboMeowCat ( talk) 18:57, 25 February 2014 (UTC)
- ok, please pardon me that i missed the emphasis. please do stop repeating yourself. again (and it is the last time I will address this), i point you to WP:WEIGHT, which is policy, and which you are ignoring. The article is very clear and unambiguous that p. use and later asthma are correlated. the points you keep bringing are the criteria that are used to argue for causation. as others have already written to you, as of the date we are writing, the mainstream view is that causation is not established and that the recommendations are unchanged. As per WP:WEIGHT, we do not give more weight to the minority view which is that causation is established. now, the mainstream view may evolve. if and when it does, we can update the article. again, please let this go already and please stop repeating yourself. the WP article has gone as far as it can on the point you care about, which at this time is not the mainstream view. the only sources that will be compelling for this, will be a change in a statement by one of the major medical bodies that we cite, or a new statement by one we don't cite yet. thanks. Jytdog ( talk) 19:26, 25 February 2014 (UTC)
I can live with the wording of the most recent revision by BoboMeowCat. If he is satisfied, we may be close to consensus. Formerly 98 ( talk) 20:37, 25 February 2014 (UTC)
- Today's statement switched back to McBride's recommendation, and is now listing only the AAP and NICE as competing views. The approach seems designed to diminish the mainstream view, but I'm not sure how that can be countered with the requirement of proving a guideline is current as of 2014, except in the cases (like AAP & NICE) where they're repeated on layperson-friendly websites which are presumed to be current. Consider the WHO or JPS, for example, who also published recommendations for paracetamol use by children without any mention of asthma or risk of asthma. WHO publishes recommendations in rarely-released books, with periodic updates in the interim, so their most recent recommendations (I think, but can't prove) are from 2005. Similar issue with the JPS's 2012 guidelines. Are we omitting them because they don't have a dumbed down website?
- Handbook: IMCI Integrated Management of Childhood Illness (PDF). World Health Organization. 2005. pp. 47, 49–50, 55, 88, 92, 97, 102, 112, 145. ISBN 92 4 154644 1.
- Ishizaki, Yuko; et al. (2012). "Japanese clinical guidelines for chronic pain in children and adolescents" (PDF). Pediatrics International. 54 (1). Japan Pediatric Society: 1–7. doi: 10.1111/j.1442-200X.2011.03543.x. ISSN 1328-8067.
- The National Health Service does have a ”consumer“ website, and I think can be added uncontroversially:
- "Painkillers, paracetamol". NHS Choices. UK National Health Service.
- I guess the reason I'm content with it is that I consider both NICE ande AAP to be the most authoritative sources by far among those listed. I may be overestimating the extent to which others will see it the way I do, but I'm getting less demanding as time goes on out of sheer exhaustion. Formerly 98 ( talk) 03:02, 26 February 2014 (UTC)
Acetaminophen & asthma
Have added that "The majority of the evidence does not; however, support a causal role." for acetaminophen based on "The weight of evidence of the collected studies in our review strongly suggests that the association of antibiotics with childhood asthma reflects various forms of bias, the most prominent of which is confounding by indication. Recent studies and meta-analyses support the same conclusion for paracetamol. " [4] Doc James ( talk · contribs · email) (if I write on your page reply on mine) 14:32, 18 May 2014 (UTC)
- You are confusing "antibiotics" with "acetaminiophen". See your edit summary over on asthma article. Additionally, the most recent studies would reflex primary research. Secondary research of multiple studies only supports this claim for antibiotics --
BoboMeowCat (
talk)
14:40, 18 May 2014 (UTC)
- Not by my reading. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 14:53, 18 May 2014 (UTC)
- You are confusing "antibiotics" with "acetaminiophen". See your edit summary over on asthma article. Additionally, the most recent studies would reflex primary research. Secondary research of multiple studies only supports this claim for antibiotics --
BoboMeowCat (
talk)
14:40, 18 May 2014 (UTC)
- BoboMeowCat can you not see that the abstract says "Recent studies and meta-analyses support the same conclusion for paracetamol."? Jytdog ( talk) 16:40, 18 May 2014 (UTC)
- Recent edit written by Jytdog and restored by DocJames not supported by the references. https://en.wikipedia.org/?title=Paracetamol&oldid=609098410
- Here’s the edit:
- “There is an association between paracetamol use and asthma but the weight of evidence of the collected studies strongly suggests that the association reflects various forms of bias, the most prominent of which is confounding by indication.[46] The majority of the evidence does not support a causal role.[47]”
- To break it down, the first part: “the weight of evidence of the collected studies strongly suggests that the association reflects various forms of bias, the most prominent of which is confounding by indication”
- It’s referenced by this source. https://www.ncbi.nlm.nih.gov/pubmed/23347656 From article abstract:
- “There is substantial epidemiological evidence in adults and children that acetaminophen use is associated with asthma symptoms. There is also a considerable body of evidence that supports a modest but consistent association of acetaminophen use in pregnancy and early infancy with asthma in later childhood. This relationship is robust to adjustment for a large range of potential confounding factors and, in some studies, shows clear evidence of a dose-dependent association but the possibility of confounding by indication has remained a concern. However, the epidemiological evidence is now compelling and there is a clear need to establish causation so that appropriate advice and interventions can be developed for children at risk of asthma. This requires randomised trials of analgesics and antipyretics, including acetaminophen, in a variety of clinical settings.”
- I'm confused how “the weight of evidence of the collected studies strongly suggests that the association reflects various forms of bias, the most prominent of which is confounding by indication”, could be concluded from this article. This article did not say the weight of the evidence suggests bias, but rather the article left bias open as a possibility. At best this seems an example of extreme WP:Cherrypicking
- The second part, “The majority of the evidence does not support a causal role” is referenced by this article https://www.ncbi.nlm.nih.gov/pubmed/23292157. The discussion section of this article says the majority of evidence does not support a causal role for antibiotics and recent studies suggest “confounding of indication” for acetaminiophen. Recent studies does not equal the majority of studies.
- If you look at the above 2 secondary sources on asthma and acetaminophen/paracetamol along with these additional secondary sources:
- It seems clear that the previous edit is does not reflect the data on the topic of paracetamol and asthma neutrally and accurately.--
BoboMeowCat (
talk)
03:45, 20 May 2014 (UTC)
- The ref says "Recent studies and meta-analyses support the same conclusion for paracetamol." It is from 2013 which is newer than 2011.
Doc James (
talk ·
contribs ·
email) (if I write on your page reply on mine)
09:22, 20 May 2014 (UTC)
- That’s referring to confounding of indication. Recent studies suggest confounding of indication may be issue with paracetamol/acetaminophen, which was reflected in my version of the edit. Also, newer doesn’t prove better, if it did, we would not have the WP:MEDRS restriction regarding primary research, which tends to be the newest research. Recent studies cannot logically reflect the majority of the evidence. Please stop restoring content not supported by the references cited.--
BoboMeowCat (
talk)
11:12, 20 May 2014 (UTC)
- Do you know what "confounding by indication" refers to? Doc James ( talk · contribs · email) (if I write on your page reply on mine) 11:29, 20 May 2014 (UTC)
- That’s referring to confounding of indication. Recent studies suggest confounding of indication may be issue with paracetamol/acetaminophen, which was reflected in my version of the edit. Also, newer doesn’t prove better, if it did, we would not have the WP:MEDRS restriction regarding primary research, which tends to be the newest research. Recent studies cannot logically reflect the majority of the evidence. Please stop restoring content not supported by the references cited.--
BoboMeowCat (
talk)
11:12, 20 May 2014 (UTC)
- The ref says "Recent studies and meta-analyses support the same conclusion for paracetamol." It is from 2013 which is newer than 2011.
Doc James (
talk ·
contribs ·
email) (if I write on your page reply on mine)
09:22, 20 May 2014 (UTC)
- It seems clear that the previous edit is does not reflect the data on the topic of paracetamol and asthma neutrally and accurately.--
BoboMeowCat (
talk)
03:45, 20 May 2014 (UTC)
- I'd suggest that the article should reflect the "average" of the last half dozen or so secondary references and not give outsized weight to the most recent one. But having said that, I have not dug into this issue again to an extent that allows me to say whether this is already the case in the version proposed by DocJames.
- With regard to the language BobMeowCat is promoting, from my POV this absolutely does not fly. Four or five editors engaged with him on the issue of the McBride review for literally thousands of words of debate just a month or two ago. The overwhelming consensus of this group was that extensively quoting the one review out of a dozen that argued for a causative relationship was undue weight. In my opinion, his current attempt to bring this back in again after a clear expression of consensus against it is just plain disruptive editing, and takes this discussion outside the realm of a mere content dispute into a violation of the behavioral guidelines. This may need to be taken up on the Admin notice board if it continues. Formerly 98 ( talk) 13:21, 20 May 2014 (UTC)
Acetaminophen Reduces Both Pain and Pleasure, Study Finds
- Thanks but we only use secondary sources generally.
Doc James (
talk ·
contribs ·
email)
07:36, 14 April 2015 (UTC)
- Original Ohio State University article handle embargoed from February last year, and the DOI for the published article in PSS. Jon ( talk) 10:14, 14 April 2015 (UTC)
- Thanks but we only use secondary sources generally.
Doc James (
talk ·
contribs ·
email)
07:36, 14 April 2015 (UTC)
Well, I added a brief entry under "Adverse Effects" with a reference. I'm not convinced it's a necessarily adverse effect, but certainly interesting :-) I used the new in-place editor to add the reference; not sure how to add multiple authors; shall amend presently with the markup editor. Jon ( talk) 10:33, 14 April 2015 (UTC)
- nether source is OK for health related content - the scientific article is a PRIMARY source (please see Wikipedia:Identifying_reliable_sources_(medicine)#Definitions) and also please see Wikipedia:Identifying_reliable_sources_(medicine)#Respect_secondary_sources, specifically about the popular media source hyping the PRIMARY source. We need to wait until this is discussed in SECONDARY source (see definitions above). Someone else already reverted the addition on these grounds.. hope that makes sense. Jytdog ( talk) 12:17, 14 April 2015 (UTC)
- I see! Fair enough so. I thought you were talking about TERTIARY sources. Jon ( talk) 13:24, 14 April 2015 (UTC)
Hyperactivity and Neural Development - Censorship
Two recent studies indicate problems in hyperactivity [1] and neural development [2] of children.
- Yeah, so I add two interesting and important new, relevant references to an article which indicates potential harm to pregnant women on the Paracetamol page. These are removed because you guys don't like primary sources? This is ridiculous and frankly an extreme case of what is wrong with Wikipedia. My wife is pregnant. I for sure want to know about potential harm of this drug. I would think as a medical professional that you would be more inspired by the "first do no harm" idea. The fact that you Wikipedia jerks are so focused on having only sources from a narrow range of whatever it takes for a given article is so frustrating. I've continued to run into this kind of thing. You would think that academic journals have taken over Wikipedia. The idea that I have actually improved the article with my additions, and that others can improve it further, has completely escaped much of the Wikipedia culture these days. Wikipedia has simply forgotten the idea that this is collaboratively edited, rather than having a coterie of people who simply reject all edits if they do not thread the eye of the needle through the dozens of acronym style guides. You guys are disgusting, really. You are standing on the shoulders of millions of edits and now you reject the very thing that got you to where you are, namely lots of collaboratively edited small improvements. Now any change has to go through hurdles that would never have created Wikipedia in the first place. The fact that you have excluded something that is evidence of significant danger to pregnant women based on this culture of exclusiveness should trouble you deeply. -- Jeffmcneill ( talk) 03:01, 27 July 2015 (UTC)
References
- ^ Liew Z, Ritz B, Rebordosa C, Lee PC, Olsen J (2014). "Acetaminophen use during pregnancy, behavioral problems, and hyperkinetic disorders". JAMA Pediatr. 168 (4): 313–20. doi: 10.1001/jamapediatrics.2013.4914. PMID 24566677.
- ^ Brandlistuen RE, Ystrom E, Nulman I, Koren G, Nordeng H (2013). "Prenatal paracetamol exposure and child neurodevelopment: a sibling-controlled cohort study". Int J Epidemiol. 42 (6): 1702–13. doi: 10.1093/ije/dyt183. PMC 3887567. PMID 24163279.
New potential source
This looks like a good source:
Should you take Tylenol, Advil, or aspirin for pain? Here's what the evidence says. (vox.com)
-- Distelfinck ( talk) 22:17, 18 August 2015 (UTC)
- That source doesn't meet WP:MEDRS, but thanks for bringing it. Jytdog ( talk) 10:41, 19 August 2015 (UTC)
- Alright. There's lots of links to scientific articles in it though, so we could use those as sources -- Distelfinck ( talk) 14:12, 19 August 2015 (UTC)
- We already comment on the issue of back pain using the high quality sources
[5]
Doc James (
talk ·
contribs ·
email)
15:32, 19 August 2015 (UTC)
- Distelfinck please do read WP:MEDRS and per Doc James the content in the article is already supported by the sources that meet MEDRS well. Jytdog ( talk) 15:39, 19 August 2015 (UTC)
External links modified
Hello fellow Wikipedians,
I have just added archive links to one external link on
Paracetamol. Please take a moment to review
my edit. If necessary, add {{
cbignore}} after the link to keep me from modifying it. Alternatively, you can add {{
nobots|deny=InternetArchiveBot}} to keep me off the page altogether. I made the following changes:
- Added archive https://web.archive.org/20130912075213/http://www.nhs.uk:80/Conditions/Flu/Pages/selectorshow.aspx?medicine=Phenylephrine/Guaifenesin/Paracetamol to http://www.nhs.uk/Conditions/Flu/Pages/selectorshow.aspx?medicine=Phenylephrine/Guaifenesin/Paracetamol
When you have finished reviewing my changes, please set the checked parameter below to true to let others know.
This message was posted before February 2018.
After February 2018, "External links modified" talk page sections are no longer generated or monitored by InternetArchiveBot. No special action is required regarding these talk page notices, other than
regular verification using the archive tool instructions below. Editors
have permission to delete these "External links modified" talk page sections if they want to de-clutter talk pages, but see the
RfC before doing mass systematic removals. This message is updated dynamically through the template {{
source check}} (last update: 5 June 2024).
- If you have discovered URLs which were erroneously considered dead by the bot, you can report them with this tool.
- If you found an error with any archives or the URLs themselves, you can fix them with this tool.
Cheers.— cyberbot II Talk to my owner:Online 16:32, 6 February 2016 (UTC)
More research needed
I am not a big fan of this bland statement as this is true for half the stuff in Wikipedia. Therefore have removed "however, further studies are needed to evaluate the validity of concerns regarding the neurological development of the offspring" Doc James ( talk · contribs · email) 09:32, 12 July 2016 (UTC)
- In this case it looks more like your opinion prevails over the conclusion of the authors.
[6]
Ekem (
talk)
17:43, 12 July 2016 (UTC)
- Not at all. User:Doc James is precisely reflecting the cited article, which says essentially "of course, our study isn't definitive (very few are), but as far as we can tell, XXX". I agree completely with Doc James's edit. -- Macrakis ( talk) 02:29, 13 July 2016 (UTC)
- Further studies, such as this? "Prenatal exposure to acetaminophen and children's language development at 30 months." [1]
Toxicity
User:Abductive your changes here and here and here are adding WP:UNDUE weight to the risks of this drug, and the content you added about "physicians have not internalized these results and continue to recommend" is unsupported editorializing. If you add this back one more time you will violate 3RR and can be blocked. Jytdog ( talk) 18:16, 16 August 2016 (UTC)
- Really? You sure are quick to dismiss the edits. Perhaps you should ask for more citations instead?
Abductive (
reasoning)
18:17, 16 August 2016 (UTC)
- This subject has been extensively discussed here on Talk. See
here and the section below that and elsewhere. The existing content is the result of careful discussion and accurately reflects the sources.
Jytdog (
talk)
18:18, 16 August 2016 (UTC)
- All you are doing is reverting, denying scientific source I added to the article. You need to read the source.
Abductive (
reasoning)
18:30, 16 August 2016 (UTC)
- In the third dif above you removed a very strong source, PMID 25851072 - a review from 2015 - and added a weak source - a hot off the presses primary source here that the field has not even had time to consider yet. This is not how we edit about medicine. See WP:MEDRS, particularly the WP:MEDREV section. Jytdog ( talk) 18:55, 16 August 2016 (UTC)
- You have now reverted a fourth time. I won't follow you over that line. Jytdog ( talk) 19:10, 16 August 2016 (UTC)
- All you are doing is reverting, denying scientific source I added to the article. You need to read the source.
Abductive (
reasoning)
18:30, 16 August 2016 (UTC)
- This subject has been extensively discussed here on Talk. See
here and the section below that and elsewhere. The existing content is the result of careful discussion and accurately reflects the sources.
Jytdog (
talk)
18:18, 16 August 2016 (UTC)
Paracetamol is generally accepted as safe during pregnancy as supported by the references provided. One of the articles does not appear to be pubmed indexed [7]? Doc James ( talk · contribs · email) 19:17, 16 August 2016 (UTC)
- Yes too new to be indexed yet! Jytdog ( talk) 20:22, 16 August 2016 (UTC)
- Just to note
there's a more recent review on the matter from last December which essentially echos the current text.
M. A. Bruhn (
talk)
21:05, 16 August 2016 (UTC)
- There's also a somewhat more recent review which states "the literature examined in this article suggests a review of the widespread opinion that acetaminophen is safe during pregnancy". I believe it might be a good time to revisit the current text in the article and make some slight alterations. M. A. Bruhn ( talk) 21:23, 16 August 2016 (UTC)
FYI this has appeared in the uk press today. - Roxy the dog™ bark 21:29, 16 August 2016 (UTC)
- When that primary study appears in a review, we can cover it. However, I'd note that the conclusion of the paper doesn't establish causality. It just points out that there is evidence against confounding factors involved in the correlation. In reality, the relationship could be causal - this isn't implausible since paracetamol's biomolecular targets are expressed in brain cells - however this has not been established yet in any research. It's important not to overstate the facts since it's also possible that there are other confounding factors (see omitted variable bias) that are unrelated to mid-/post-pregnancy paracetamol use and partner paracetamol use. Seppi333 ( Insert 2¢) 19:34, 17 August 2016 (UTC)
Article on Acetaminophen and Behavioural disorders
A very large study suggesting that Acetaminophen or Paracetamol use doing pregnancy may be responsible for ADHD and other disorders in childrem
http://www.ncbi.nlm.nih.gov/pubmed/24566677Cite error: There are <ref> tags on this page without content in them (see the
help page).
This should be part of the discussion on this drug. 2602:306:BCED:1070:6809:6C22:4C3:FD07 ( talk) 17:41, 22 August 2016 (UTC)
- 2 year old study that has been discussed to death here. Jytdog ( talk) 17:45, 22 August 2016 (UTC)
Requested move 16 November 2016
- The following is a closed discussion of a requested move. Please do not modify it. Subsequent comments should be made in a new section on the talk page. Editors desiring to contest the closing decision should consider a move review. No further edits should be made to this section.
The result of the move request was: Not moved per WP:SNOW. ( non-admin closure) Zarcadia ( talk) 20:50, 16 November 2016 (UTC)
Paracetamol →
Para-acetylaminophenol –
WP:COMMONALITY ; this should not favour either British English (paracetamol) or North American English (acetaminophen), instead it should use the origin term that paracetamol (para-acetylaminophenol) and acetaminophen (para-acetylaminophenol) and Tylenol (para-acetylaminophenol) are abbreviations of, namely "
para-acetylaminophenol" --
65.94.171.217 (
talk)
04:30, 16 November 2016 (UTC)
Survey
- Feel free to state your position on the renaming proposal by beginning a new line in this section with
*'''Support'''or*'''Oppose''', then sign your comment with~~~~. Since polling is not a substitute for discussion, please explain your reasons, taking into account Wikipedia's policy on article titles.
- Support I am the nominator; no biases in the dialect used, and "P-acetylaminophenol" is not too uncommon either. -- 65.94.171.217 ( talk) 04:32, 16 November 2016 (UTC)
- Oppose not even close to WP:COMMONNAME. Not in popular use nor in the literature. This will be a snow close. Jytdog ( talk) 05:01, 16 November 2016 (UTC)
- Oppose as Jytdog In ictu oculi ( talk) 07:47, 16 November 2016 (UTC)
- Oppose, totally inappropriate suggestion, please close per WP:SNOW. MrStoofer ( talk) 09:33, 16 November 2016 (UTC)
- Snowpose. Paracetamol is not limited to British English, but is actually the international nonproprietary name and far more common than this chemical monstrosity. -- HyperGaruda ( talk) 18:26, 16 November 2016 (UTC)
Discussion
- Any additional comments:
- The above discussion is preserved as an archive of a requested move. Please do not modify it. Subsequent comments should be made in a new section on this talk page or in a move review. No further edits should be made to this section.
INN
What is the INN of paracetamol? - DePiep ( talk) 21:57, 25 November 2016 (UTC)
- I think it is paracetamol. Doc James ( talk · contribs · email) 23:53, 25 November 2016 (UTC)
Cochrane blog
User:Jtamad why are you adding a blog source to a medical section? Jytdog ( talk) 03:57, 19 August 2017 (UTC)
References
- ^ Bornehag, C.-G.; Reichenberg, A.; Hallerback, M. Unenge; Wikstrom, S.; Koch, H.M.; Jonsson, B.A.; Swan, S.H. "Prenatal exposure to acetaminophen and children's language development at 30 months". European Psychiatry. doi: 10.1016/j.eurpsy.2017.10.007.
Effectiveness in children
There is a blanket statement at the start of this article which seems to be entirely out of place and largely false.
"There is poor evidence for fever relief in children."
This links to a meta-study that is 15 years old, that contains a very small sample size.
Even as somebody who is not medical, this statement seems absurd, given that many people have success with paracetamol for fever relief in children. Even my local world renowned children's hospital (Royal Children's Hospital in Melbourne, Australia) have guidelines written in 2013 that recommend the use of paracetamol for fever relief.
http://www.rch.org.au/kidsinfo/fact_sheets/Pain_relief_for_children_-_Paracetamol_and_Ibuprofen/
I would think it prudent to just remove this sentence altogether, as it is totally out of place and at odds with common sense. — Preceding unsigned comment added by Jessejackson100 ( talk • contribs) 02:49, 27 May 2017 (UTC)
Jessejackson100 ( talk) 02:56, 27 May 2017 (UTC) JJ
- I doubt much has changed since 2002. Do you have a source that says their is good evidence? Temps go up and they come down, thus one needs a placebo controlled trial. Doc James ( talk · contribs · email) 03:38, 27 May 2017 (UTC)
- But you understand what I'm saying here? The tone of that sentence is such that a casual reader would take it to mean that paracetamol 100% does not work in children. At least that's what I hear when I see the words "poor evidence". I am a sample size of 1, but I have seen it 100% work in a child on multiple occasions. This sentence as it is currently structured doesn't seem to allow for the fact that in some circumstances, it works. This Wikipedia article is the first I've ever heard of this, which is contrary to the advice I've been given by every medical doctor I've been in contact with on every occassion that I've had a sick child with a fever.
- A search on Google scholar for articles relating to fever management in children brings up a number of more recent articles, many which are comparing paracetamol to ibuprofen in children. They all seem to agree that ibuprofen is more effective, but none of them state that paracetamol plain doesn't work. It appears that there are limited studies though in this field, and that single meta study with n = 1500ish doesn't seem to warrant the finality of this statement.
Jessejackson100 (
talk)
10:29, 27 May 2017 (UTC)
- I have seen doing nothing work frequently as well. Indeed ibuprofen appears to work better than acetaminophen. The question is does acetaminophen work better than placebo?
- Basically we need properly done RCTs with the comparison being placebo to show whether or not paracetamol works. The little evidence there is says it does not.
Doc James (
talk ·
contribs ·
email)
17:26, 27 May 2017 (UTC)
- I just did a mini review of the literature and I don't see many new RCTs on this topic. I was initially a bit puzzled why I didn't see Cochrane publish an updated review but I suppose it wouldn't be very meaningful since it would likely just reiterate the findings from the 2002 review since there isn't much new data. TylerDurden8823 ( talk) 18:01, 28 October 2017 (UTC)
- A search on Google scholar for articles relating to fever management in children brings up a number of more recent articles, many which are comparing paracetamol to ibuprofen in children. They all seem to agree that ibuprofen is more effective, but none of them state that paracetamol plain doesn't work. It appears that there are limited studies though in this field, and that single meta study with n = 1500ish doesn't seem to warrant the finality of this statement.
Jessejackson100 (
talk)
10:29, 27 May 2017 (UTC)
Effectiveness
The article seems very weak on evidence that paracetamol really has any pain-relieving effect at all. Largely the article just seems to take it for granted that it does actually work, with the exception of a couple of special applications where efficacy is questioned. For me the effect of paracetamol on any type of pain (that I have tested) is zero to undetectable. I know that I am not unique in this respect. 86.191.44.105 ( talk) 04:31, 2 February 2017 (UTC)
- There is evidence for some stuff. But yes it is a weak pain medication. Doc James ( talk · contribs · email) 05:54, 2 February 2017 (UTC)
- Agreed, it's a low-strength analgesic. TylerDurden8823 ( talk) 18:02, 28 October 2017 (UTC)
| This is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 | Archive 2 | Archive 3 | Archive 4 | Archive 5 |
Disruptive Activity
![]() Please stop your
disruptive editing. If you continue to
vandalize Wikipedia, as you did at
Paracetamol, you may be
blocked from editing. --
CFCF
🍌 (
email)
04:10, 27 July 2015 (UTC)
Please stop your
disruptive editing. If you continue to
vandalize Wikipedia, as you did at
Paracetamol, you may be
blocked from editing. --
CFCF
🍌 (
email)
04:10, 27 July 2015 (UTC)
- Yeah, so I add two interesting and important new, relevant references to an article which indicates potential harm to pregnant women on the Paracetamol page. These are removed because you guys don't like primary sources? This is ridiculous and frankly an extreme case of what is wrong with Wikipedia. My wife is pregnant. I for sure want to know about potential harm of this drug. I would think as a medical professional that you would be more inspired by the "first do no harm" idea. The fact that you Wikipedia jerks are so focused on having only sources from a narrow range of whatever it takes for a given article is so frustrating. I've continued to run into this kind of thing. You would think that academic journals have taken over Wikipedia. The idea that I have actually improved the article with my additions, and that others can improve it further, has completely escaped much of the Wikipedia culture these days. Wikipedia has simply forgotten the idea that this is collaboratively edited, rather than having a coterie of people who simply reject all edits if they do not thread the eye of the needle through the dozens of acronym style guides. You guys are disgusting, really. You are standing on the shoulders of millions of edits and now you reject the very thing that got you to where you are, namely lots of collaboratively edited small improvements. Now any change has to go through hurdles that would never have created Wikipedia in the first place. The fact that you have excluded something that is evidence of significant danger to pregnant women based on this culture of exclusiveness should trouble you deeply. -- Jeffmcneill ( talk) 06:21, 27 July 2015 (UTC)
- Jeffmcneill I'm sorry that I've upset you, but the fact is we get hundreds upon hundreds of poor quality changes every day. That is why we've written WP:MEDRS which I pointed to when I reverted you. There is also an excellent essay on why we adhere so strongly to it at WP:WHYMEDRS. The fact is that many primary studies are either performed on mice or on very small populations so that their results can't be transferred into clinical practise. MEDRS is no catch all, but it helps us and makes patrolling many articles and removing citations from the daily mail easier. I would also like to point out that we are working on getting these types of warnings into our articles automatically, for example by having FDA warnings automatically added.
- These were both large studies not having anything to do with mice. These rules are not useful, and essay reading should not be a requirement for submitting actual value to the article. Again, how would Wikipedia even exist if this kind of hurdle was required to get it started? This behavior is not sustainable. Eventually the remaining admins will actually reach the end of their productive lives and then what, Wikipedia will live on as a set of revert bots? Most likely. -- Jeffmcneill ( talk) 11:54, 27 July 2015 (UTC)
- I understand it may feel as if you're being reverted by a faceless mass, but I assure you if you had simply taken up the discussion it would have been far more likely to be productive. -- CFCF 🍌 ( email) 11:10, 27 July 2015 (UTC)
- This isn't about my feelings, it is about your behavior. You revert me with no reason, then start quoting this bureaucratic nonsense, then threaten me with banning due to my disruptive editing. This is why Wikipedia is dying, cannibalizing its editors and edits in a Kafkaesque farce. Congratulations, I'm sure your no-doubt proper and uplifting ZYZZYXRD will be cited upon its demise. You may want to try and comprehend your own actions, and not my feelings. See < http://www-users.cs.umn.edu/~halfak/publications/The_Rise_and_Decline/>. -- Jeffmcneill ( talk) 11:49, 27 July 2015 (UTC)
Asthma
There certainly seems to be an epidemiological association here, but I don't think consensus view is favors causation to the extent of the language that was added.
Here are the papers I found:
1) http://www.ncbi.nlm.nih.gov/pubmed/20933592: " At present, the evidence is inconclusive that any such association is causal."
2) http://www.ncbi.nlm.nih.gov/pubmed/23547988 " Is acetaminophen a real asthma promoter or an innocent bystander?"
3) http://www.ncbi.nlm.nih.gov/pubmed/23347656 "However, the epidemiological evidence is now compelling and there is a clear need to establish causation so that appropriate advice and interventions can be developed for children at risk of asthma. This requires randomised trials"
4) http://www.ncbi.nlm.nih.gov/pubmed/23292157 "Truly indicated antibiotics should not be withheld from infants or young children for fears they might develop asthma. Likewise, there is no sound reason to replace paracetamol as the preferred pain relief and fever medication in this age group."
5) http://www.ncbi.nlm.nih.gov/pubmed/23253685: "Causality cannot be established from observational studies because of the arguable presence of many confounding factors and biases. Randomised trials are needed to disclose the nature of the association"
6) http://www.ncbi.nlm.nih.gov/pubmed/21505328 "Several studies have shown an association between acetaminophen use during pregnancy and allergic diseases in the offspring. Furthermore, this association has also been found between early exposure and recent exposure to the drug and several allergic conditions. However, other studies did not confirm those associations."
Extensively quoting from what appears to be the single review of this area that unambiguously concludes a causative relationship is undue weight. Furhtermore, offering treatment guidance to avoid the use of acetominophen goes well outside published treatment guidelines and regulatory actions. NPOV requires that space alloted to different opinions should reflect their acceptance among experts. The modified language of this section does not do that. Formerly 98 ( talk) 05:03, 20 February 2014 (UTC)
- The epidemiological association between paracetamol and asthma is well established. The numerous factors indicating this association detailed and properly cited. Sources all peer reviewed medical journal articles.
- Concerned that this properly cited information from multiple credible sources has been repeatedly edited/deleted
- Sources: [1] [2] [3] [4]
- ^ McBride, J. T. (2011). "The association of acetaminophen and asthma prevalence and severity". Pediatrics. 128 (6): 1181–5. doi: 10.1542/peds.2011-1106. PMID 22065272.
- ^ Eneli, I; Sadri, K; Camargo Jr, C; Barr, R. G. (2005). "Acetaminophen and the risk of asthma: The epidemiologic and pathophysiologic evidence". CHEST Journal. 127 (2): 604–12. doi: 10.1378/chest.127.2.604. PMID 15706003.
- ^ Beasley, R; Clayton, T; Crane, J; von Mutius, E; Lai, C. K.; Montefort, S; Stewart, A; ISAAC Phase Three Study Group (2008). "Association between paracetamol use in infancy and childhood, and risk of asthma, rhinoconjunctivitis, and eczema in children aged 6-7 years: Analysis from Phase Three of the ISAAC programme". The Lancet. 372 (9643): 1039–48. doi: 10.1016/S0140-6736(08)61445-2. PMID 18805332.
- ^ Farquhar, H; Stewart, A; Mitchell, E; Crane, J; Eyers, S; Weatherall, M; Beasley, R (2010). "The role of paracetamol in the pathogenesis of asthma". Clinical & Experimental Allergy. 40 (1): 32–41. doi: 10.1111/j.1365-2222.2009.03378.x. PMID 20205695.
- Epidemiological associations do not prove causation by themselves. This sort of evidence is very similar to that which for many years was cited as evidence that post menopausal hormone replacement therapy prevents heart attacks in women. The Women's health initiative trial showed that the reduced cardiovascular events were not due to HRT, which actually increases CV risk, but to differing baseline characteristics of women who do and don't use HRT. That's why I'm so forceful about differentiating epidemiological association from causation here.
- I've cited about half a dozen articles in which experts state that they do not consider causation proven, including a few that state it is unlikely. Among the studies you have cited, the author of the first considers causality essentially proven. The second states that there is a "possible link". The third states that "paracetamol might be a risk factor". The fourth states that it is a "putative risk factor".
- So from among the 10 references that the two of us have found on this subject, one considers it proven that paracetamol causes asthma, and 9 draw conclusions varying from "it is unlikely that paracetamol causes asthma" to "it is likely but unproven". I don't understand why you have chosen to quote so extensively from the single article that considers the relationship essentially proven, when this seems to me to clearly be a minority (10%) viewpoint.
- Nor have I deleted the reference to asthma. I've merely toned down the statements regarding causation to match what seems to me to be mainstream opinion.
- Could we adjust the language to some mid point between what I had and your most recent version? Thanks Formerly 98 ( talk) 09:40, 20 February 2014 (UTC)
Nowhere in my edit was it claimed epidemiological associations prove causation. Indicated epidemiological association between paracetamol use and asthma well established. Detailed factors which firmly establish epidemiological association. Cited multiple references to peer reviewed medical journals supporting strong epidemiological association between paracetamol use and asthma. Epidemiological evidence invaluable and used to establish link between cigarette smoking and lung cancer. Added link to Epidemiology wiki page. Additionally, I left in your edit regarding possible debate word for word. Please stop deleting my accurate and properly referenced content. — Preceding
unsigned comment added by
BoboMeowCat (
talk •
contribs)
11:01, 20 February 2014 (UTC)
- Yes lots of reviews that discuss. Maybe be useful in a "research" section at the bottom of the article. I have removed the copy and pasted content as it is a copyright violation. Have also summarized in general terms and removed the primary research. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 14:13, 20 February 2014 (UTC)
I have compromised and cooperated fully. Edits regarding possible debate and possible confounding by indication were left in place word for word. Additionally, I’ve added a statement which explicitly indicates epidemiological associations do not prove causation. I had already linked to Epidemiology Wiki page for clarity. Despite this, my accurate and properly sourced information regarding strong epidemiological link to asthma has been repeatedly deleted. Because of this repeated occurrence, I’ve become concerned that “compromise” is being misused to mean censorship of accurate and properly referenced information regarding paracetamol’s well established epidemiological link to asthma.
My text was never copied and pasted, as words were changed. Wording has now been extensively changed to remove any remote hint of copyright violation. I’m going to ask again that this accurate and properly referenced information not be deleted, as repeatedly doing so suggests censorship of accurate information regarding epidemiological link to asthma and possible conflict of interest editing. –BoboMeowCat
- Bob, I'll wait for JMH649 to comment, but from my POV the issue with your new edit is the same as the old one. There are 10 relevant citations regarding this association, of which more than half say the case for causality is weak, and all but one of the remainder explicitly state that it is unproved. But while giving a nod to the idea that "association does not prove causation", you go on to present a counterpoint that lists out a long line of reasoning supporting the idea that it is essentially proven. Only one of 10 references supports this POV. You follow that up with a recommendation to avoid paracetamol in children that does not appear in any of the other 9 references (one of which recommends exactly the opposite).
- Pasting into Word, I count 143 words describing the single paper that supports your POV, and 60 words describing the 9 papers that don't. This is pretty much the definition of WP:RSUW. Its not that what you've said isn't a correct description of what is said in a WP:MEDRS compliant source. Its that you give undue space to a minority point of view relative to the majority POV. And that's equally against the rules here. Formerly 98 ( talk) 22:32, 21 February 2014 (UTC)
I'd like to ask that you please stop pretending I'm asserting causality rather than sharing accurate information regarding a very well established epidemiological association between paracetamol and asthma (which I followed with a detailed explanation of what makes this association so well established). I cited many sources to support. Also, please note explicit statement in my edit which indicates epidemiological associations do not prove causation. At this point, I'm fully expecting JMH649 will support you, as you summoned him in the first place, and his edits were extremely similar to your edits. I'm concerned that there appears to be an effort to censor accurate and properly referenced information, suggesting conflict of interest editing. If it is felt that information from any of your above mentioned sources is relevant, I'd like to ask you to please add that information as a separate edit, and refrain from again deleting accurate and properly referenced content. -- BoboMeowCat ( talk) 23:04, 21 February 2014 (UTC)
- Bob, all I'm asking is that you look at the paragraph you wrote and ask yourself if the average reader isn't going to walk away saying "wow, with that detailed list of points on how strongly the evidence favoring causation is, who are those nuts who aren't yet convinced that paracetamol causes asthma?" You've given a detailed account of one side of the argument and noted only that some don't agree with it.
- In fact, if you look at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3651816/ this author has provided a point by point rebuttal of each of the points that you quote from the McBride article. I could add these, but then the whole section becomes a rambling digression. It seems best just to keep it short since it is an unsettled issue.
- It would also be very helpful if you would lay off the accusations and abide by WP:GF. One could just as easily accuse you of being an agent of the companies that manufacture ibuprofen, especially as the only subject you have engaged on in some 35 Wikipedia edits is the role of acetominophen in asthma. As you can see, these sorts of personal attacks don't lead anywhere.
- Jmh by the way is the founder of the Wikipedia Medicine Project and the most senior person addressing medical issues in the organization. I thought he would probably support my position (because I think I am right), but he has overruled me on a number of occasions. He's not so much an ally of mine as someone who has broad overall responsibility for the medical content of the encyclopedia. I asked him to mediate as we were not reaching agreement among ourselves.
Formerly 98 (
talk)
00:54, 22 February 2014 (UTC)
- We are to summarize. The ref you removed was newer. So thanks Formerly for restoring the better version IMO. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 01:43, 22 February 2014 (UTC)
- Jmh by the way is the founder of the Wikipedia Medicine Project and the most senior person addressing medical issues in the organization. I thought he would probably support my position (because I think I am right), but he has overruled me on a number of occasions. He's not so much an ally of mine as someone who has broad overall responsibility for the medical content of the encyclopedia. I asked him to mediate as we were not reaching agreement among ourselves.
Formerly 98 (
talk)
00:54, 22 February 2014 (UTC)
Formelly 98 and Doc James, I’d like you to ask yourselves why you (or anyone for that matter) would want to censor accurate information regarding paracetamol’s very strong, repeatedly demonstrated, epidemiological link to asthma? If accurate and properly referenced information (from 5 credible sources, 2 of which were reviews of many studies) makes people think, “wow, this very well may be a concern”, then it seems that accurate information should not be censored by Wikipedia. I have browsed multiple medication pages on Wikipedia and browsed multiple edits. It appears that conflict of interest edits, on medication pages in particular, are common on Wikipedia. Such edits repeatedly downplay potential health concerns of medications. These edits appear to be made, in large part, by individuals with known or likely ties to the pharmaceutical industry.
Please add any properly referenced additional information and/or properly referenced rebuttals, as a separate edit. Again, please refrain from deleting accurate and properly referenced content, because censorship of this accurate information regarding paracetamol's well established epidemiological link to asthma seems to undermine the credibility and utility of Wikipedia. -- BoboMeowCat ( talk) 02:56, 22 February 2014 (UTC)
- Non-medical professional here, just weighing in with a fresh set of eyes. Bobmeowcat's most recent version did give the impression that the causal link was fairly well established ("not proved; HOWEVER!") , and I would infer a "suggested" medical recommendation in a reputable encyclopedia to be based on reasonably established scientific opinion. Granted, this is Wikipedia, and only fools would treat it as reputable, but we should still strive for accuracy and balance, particularly on issues of medical advice.
- BoboMeowCat, I realize this was your first foray into editing a Wikipedia article, at least with a user account, and it can seem like people are ganging up when you're making a sincere effort to improve the article. However, editors of medical articles are particularly cautious about controversial information based on isolated medical studies, and your contribution is exactly that. If you haven't already, I'd really suggest you take a look at Wikipedia's guidance on reliable sources for medical topics, at Wikipedia:MEDRS, particularly the opening section (the rest of it you could skim or skip, or read for clarification on cretain points). Other topics tend to be less stringent, and outside of academia there generally aren't equivalents of literature/systematic reviews, so there is more leeway in introducing non-mainstream opinions.
- Hmm...as I was typing this, I see that you reverted the reversions again. With all due respect, until there is a resolution on this issue, the controversial information should be removed. Jmh649 was asked to provide outside guidance on the issue. The short version is non-controversial, and does address the unestablished possibilty of causation. More importantly, be aware of the three revert rule ( WP:3RR) from the article on WP:EDITWARRING:
Bob we are to write in easy to understandable text. What you have added is much less understandable than what was there before. We all agree that there is an association. Is there proven causation? No and we should all be able to agree on that. That requires an RCT. One has not yet been done. Thus the association is tentative as it could be due to confounders. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 04:25, 22 February 2014 (UTC)
- Agyle, if accurate properly referenced information leads people believe this is cause for concern, that simply shows the evidence is strong and compelling. You appear to be arguing this evidence needs to be censored because it is too compelling. Additionally, this is not based on isolated medical studies. My current edit includes 11 references from peer reviewed medical journals including multiple articles which review numerous studies.-- BoboMeowCat ( talk) 15:29, 23 February 2014 (UTC)
Jmh649, only including information which suggests link not valid, while disallowing information which strongly suggests link valid, does not reflect neutrality. It is not balanced. The references to 11 primary and secondary sources included to illustrate that my edit does not represent "undue weight" material and my edit not based on "isolated studies". Regardless, accurate and extensively well referenced content again deleted, and I've been threatened with banning, if I were to restore this content. Please note, I've left in place your edits regarding possible doubt word for word. I have never deleted any of your or Formely 98's content. It is becoming clear that only information regarding doubt of association well be maintained, while all evidence suggesting link valid will be deleted. -- BoboMeowCat ( talk) 18:18, 23 February 2014 (UTC)
- There is an association. Now we need an RCT to look at the question. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 20:48, 23 February 2014 (UTC)
- Jmh649, I have zero objection to the addition of a statement regarding lack of RCT. If such a statement were added, I would not delete (as I have deleted zero content thus far, while my content repeatedly deleted). However, it does seem some would suggest ethical concerns regarding RCT in human pediatric population. Given the varied and abundant evidence linking paracetamol to asthma, such a study may be more ethical in animal model initially. --
BoboMeowCat (
talk)
21:24, 23 February 2014 (UTC)
- Wow you have obviously made up your mind. Anyway Wikipedia will update its content when more evidence is out. Right now all we have is an "association".
- We do have this 2013 review "there is no sound reason to replace paracetamol as the preferred pain relief and fever medication in this age group." [2]
- I see no reliable source claiming that acetaminophen causes asthma. Because of course currently the evidence is too weak to say it does. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 21:37, 23 February 2014 (UTC)
- Jmh649, I have zero objection to the addition of a statement regarding lack of RCT. If such a statement were added, I would not delete (as I have deleted zero content thus far, while my content repeatedly deleted). However, it does seem some would suggest ethical concerns regarding RCT in human pediatric population. Given the varied and abundant evidence linking paracetamol to asthma, such a study may be more ethical in animal model initially. --
BoboMeowCat (
talk)
21:24, 23 February 2014 (UTC)
- I have only "made up my mind" that the 11 studies referenced exist and have indicated the findings detailed (yet these findings have been repeatedly deleted). Interestingly, those who objected to the inclusion of this accurate content seem to have "made up minds", in a sense, because in this very talk section, it has been repeatedly conveyed to me that the evidence is too compelling to include.
- Additionally, a comprehensive review of asthma in pediatric population concluded: "Until future studies document the safety of this drug, children with asthma or at risk for asthma should avoid the use of acetaminophen"
- http://pediatrics.aappublications.org/content/early/2011/11/04/peds.2011-1106.full.pdf
- With your recent edit, you indicated the link may be due to confounding by indication (ie due to medications or illness coinciding with paracetamol usage). Evidence presented for this POV weaker and less well referenced, yet maintained, while more thoroughly referenced information deleted. Lack of neutrality/balance in the paracetamol asthma section troubling. -- BoboMeowCat ( talk) 23:04, 23 February 2014 (UTC)
- Bob, in spite of our disagreements, I think everyone here has been fairly diplomatic and respectful to you. But you seem locked into the idea that anyone who disagrees with you is an agent of the Evil Empire, and openly make accusations of bad faith as your primary tautological tool. As you can see, these types of tactics are not very successful here.
- I'd urge you to try a different tack. The current approach is not likely to achieve your goals. Formerly 98 ( talk) 23:12, 23 February 2014 (UTC)
- Instead of accusing me of wearing a tin foil hat, why not respond to my concerns. Why was less well referenced content regarding possible confounding by indication maintained, while more thoroughly referenced content suggesting valid link deleted? This does not seem to represent balance/neutrality. -- BoboMeowCat ( talk) 23:36, 23 February 2014 (UTC)
Hey User:BoboMeowCat. It appears that this is how you wish the section to appear. One of things we pay mind to is WP:WEIGHT. Can you please justify giving this section, which concerns an association and not an actual risk, equal weight with the liver toxicity section, which is an actual risk? The kind of argument that would be compelling, would be bringing a recent review article on overall acetaminophen toxicity that gives this association as much or more weight as liver toxicity. Thanks. Jytdog ( talk) 00:30, 24 February 2014 (UTC)
- We could summarize this as "A 2013 review concluded that paracetamol is perfectly appropriation for use in children at risk for asthma while 2011 review recommended that this group should avoid its use until there is further evidence" Anyway have added. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 00:33, 24 February 2014 (UTC)
- "Perfectly safe" does not seem to represent a balanced or neutral point of view. Additionally, presenting the information with the dates in this manner seems potentially misleading. It could easily be misinterpreted as suggesting the 2013 paper involved research demonstrating paracetamol's safety, therefore resolving the concerns brought up in the 2011 review, while this is not the case. --
BoboMeowCat (
talk)
01:08, 24 February 2014 (UTC)
- Yes we did not say "Perfectly safe"
Doc James (
talk ·
contribs ·
email) (if I write on your page reply on mine)
01:23, 24 February 2014 (UTC)
- Noted. You wrote "perfectly appropriate", which also does not seem balanced or neutral. — Preceding
unsigned comment added by
BoboMeowCat (
talk •
contribs)
01:34, 24 February 2014 (UTC)
- Yes because most of the literature still agrees that acetaminophen is "perfectly appropriate" Thus this wording is perfectly appropriate. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 01:45, 24 February 2014 (UTC)
- Noted. You wrote "perfectly appropriate", which also does not seem balanced or neutral. — Preceding
unsigned comment added by
BoboMeowCat (
talk •
contribs)
01:34, 24 February 2014 (UTC)
- Yes we did not say "Perfectly safe"
Doc James (
talk ·
contribs ·
email) (if I write on your page reply on mine)
01:23, 24 February 2014 (UTC)
- Jytdog, The difference is the liver toxicity section doesn't include text saying this is an epidemiological association which does not prove causation. Anyway, to clarify, the lack of balance/neutrality I was referring to was within the asthma subsection. In that subsection, only information suggesting link to asthma invalid included (ie due to medications or illness coinciding with paracetamol usage) while all evidence suggesting it may be a true link deleted, despite the fact that this evidence was referenced by 11 solid sources, including primary and secondary research. The claim regarding potential confounding by indication less well referenced, yet maintained. Lack of balance/neutrality --
BoboMeowCat (
talk)
01:20, 24 February 2014 (UTC)
- Thanks for responding, but that is not actually a response to my question about weight. (it is a response to why you want the content you want) Would you please respond to the question about weight? if you don't understand the question, please ask me to clarify it, thanks Jytdog ( talk) 01:24, 24 February 2014 (UTC)
- "Perfectly safe" does not seem to represent a balanced or neutral point of view. Additionally, presenting the information with the dates in this manner seems potentially misleading. It could easily be misinterpreted as suggesting the 2013 paper involved research demonstrating paracetamol's safety, therefore resolving the concerns brought up in the 2011 review, while this is not the case. --
BoboMeowCat (
talk)
01:08, 24 February 2014 (UTC)
- The American Pediatric Association recommends acetominophen for treating fever in children as of the May 2013 update of its website for parents.
http://www.healthychildren.org/English/safety-prevention/at-home/medication-safety/Pages/Acetaminophen-for-Fever-and-Pain.aspx. So it still seems to me that giving equal weight to a paper that suggests avoiding it is a little much. Nonetheless, if we can put this to bed I am fine with the current language. Thanks to everyone who worked on this, and especially to DJ, who put in a lot of time to mediate.
Formerly 98 (
talk)
01:31, 24 February 2014 (UTC)
- Yes agree we might currently be giving too much weight to the 2011 paper. Do we have a statement from the AAP we could add? Doc James ( talk · contribs · email) (if I write on your page reply on mine) 01:48, 24 February 2014 (UTC)
- The American Pediatric Association recommends acetominophen for treating fever in children as of the May 2013 update of its website for parents.
http://www.healthychildren.org/English/safety-prevention/at-home/medication-safety/Pages/Acetaminophen-for-Fever-and-Pain.aspx. So it still seems to me that giving equal weight to a paper that suggests avoiding it is a little much. Nonetheless, if we can put this to bed I am fine with the current language. Thanks to everyone who worked on this, and especially to DJ, who put in a lot of time to mediate.
Formerly 98 (
talk)
01:31, 24 February 2014 (UTC)
- Nice find! I just took my shot at crafting some language. It seems pretty clear that expert opinion is divided because there is lack of sufficient data, and in my view, the best Wikipedia can do is clearly acknowledge that. Let me know what you all think. Formerly, I used the section from the APA on OTC medicine in general, as it makes it clear that they do not drive parents toward ibuprofen over acetaminophen. Jytdog ( talk) 01:56, 24 February 2014 (UTC)
Simplier
This sentence is a little long "As of 2014, because there is insufficient data to determine if paracetamol use by pregnant women and young children causes asthma, [1] and there are different approaches to risk management, expert opinion is divided as to whether paracetamol should continue to be administered to pregnant women and children as it has in the past, [2] [3] whether paracetamol administration should be limited to cases where there is no good substitute, such as in infants younger than 3 months, [4] or if its use should be avoided until its safety is proven. [5]" Could use some simplification. The AAP deems acetaminophen to be appropriate to use to help with confort in children. [3]. The community is not exactly divided. Those recommending acetaminophen not be used are definitely the smaller group. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 02:03, 24 February 2014 (UTC)
- Hey DocJames. What I hear you saying, is the most relevant "major medical or scientific body" (to cite MEDRS) has not changed its opinion, and that is the best source to determine what the mainstream view is. True? If so, that makes sense and makes it clear that we give 'no change' the greater weight. I changed it accordingly:
- "As of 2014, the recommendations for acetaminophen use have not changed [6] but some experts have recommended restricting or avoiding its use in children and pregnant women. [7] [8]" Jytdog ( talk) 02:31, 24 February 2014 (UTC)
-
^ Cite error: The named reference
Hendersonwas invoked but never defined (see the help page). -
^ Heintze, K (2013 Jun). "The case of drug causation of childhood asthma: antibiotics and paracetamol". European journal of clinical pharmacology. 69 (6): 1197–209.
PMID
23292157.
{{ cite journal}}: Check date values in:|date=( help); Unknown parameter|coauthors=ignored (|author=suggested) ( help) - ^ American Academy of Pediatrics Last Updated July 10, 2013 Common Over-the-Counter Medications Page accessed February 23, 2014
- ^ Martinez-Gimeno A, García-Marcos L. The association between acetaminophen and asthma: should its pediatric use be banned? Expert Rev Respir Med. 2013 Apr;7(2):113-22. PMID 23547988
-
^ McBride, JT (2011 Dec). "The association of acetaminophen and asthma prevalence and severity". Pediatrics. 128 (6): 1181–5.
PMID
22065272.
{{ cite journal}}: Check date values in:|date=( help) - ^ American Academy of Pediatrics Last Updated July 10, 2013 Common Over-the-Counter Medications Page accessed February 23, 2014
- ^ Martinez-Gimeno A, García-Marcos L. The association between acetaminophen and asthma: should its pediatric use be banned? Expert Rev Respir Med. 2013 Apr;7(2):113-22. PMID 23547988
-
^ McBride, JT (2011 Dec). "The association of acetaminophen and asthma prevalence and severity". Pediatrics. 128 (6): 1181–5.
PMID
22065272.
{{ cite journal}}: Check date values in:|date=( help)
- Might be good to look at the recommendations of whatever the European equivalent of the AAP is. Having put this much time into this, we might as well do everything possible to reach a definitive conclusion. Formerly 98 ( talk) 02:41, 24 February 2014 (UTC)
- dug up the most recent EMA statement, which I got off the UK NHS press release reacting to recent data, which I also linked to. Jytdog ( talk) 07:18, 24 February 2014 (UTC)
- OK, so hopefully this issue is laid to rest now.
Jytdog (
talk)
07:18, 24 February 2014 (UTC)
- Current text: "There is an association between paracetamol use and asthma but it is unclear if it has a role in causing asthma.[42] As of 2014, the recommendations for acetaminophen use have not changed[43][44][45][46][47]:6-7 but some experts have recommended not using it in children and pregnant women.[48][49]" What recommendations? Changed from what? "Using it in..." seems like odd phrasing; "using it to treat..." seems more natural, although it still conveys a sense of something being done to them by someone else, which makes some sense for children, but not adults in countries where it's generally used without medical supervision; could switch to "...recommend X should not use Y" or something. Also, any chance "some experts" could be give any kind of indication of whether this was a common or obscure view? Citation [49], to my understanding, suggested only that children with asthma or at risk of asthma should avoid use of paracetamol, and said nothing about children in general, or pregnant women. Citation [48] has a worthless abstract and I'm not paying $84 to rent the full text for 24 hours. :-) If someone would quote the relevent sentence or two from the conclusion I'd sure appreciate it, for example [49] says “Until future studies document the safety of this drug, children with asthma or at risk for asthma should avoid the use of acetaminophen.” –– Agyle ( talk) 12:11, 24 February 2014 (UTC)
- Thanks for this helpful feedback. Ref 49 is Mcbride, who takes the risk very seriously - in the body of the article he writes: "At present, however, I need further studies not to prove that acetaminophen is dangerous but, rather, to prove that it is safe. Until such evidence is forthcoming, I will recommend avoidance of acetaminophen by all children with asthma or those at risk for asthma and will work to make patients, parents, and primary care providers aware of the possibility that acetaminophen is detrimental to children with asthma. " Ref 48 is Martinez-Gimeno, which says:
Expert commentary
Too liberal use of acetaminophen in childhood should no longer be recommended. There is a good deal of evidence suggesting that acetaminophen exposure is associated to the development of wheezing disorders and may increase its clinical manifestations in those children who already suffer them. Although the possibility still exists that acetaminophen is actually an innocent bystander, limiting its use to clinical situations in which no other alternatives remain offers practicing pediatricians a great opportunity to decrease wheezing incidence and morbidity in childhood with this simple and low-cost measure. Meanwhile, regulatory agencies should do their part and seriously reconsider the safety profile of acetaminophen and promote new and more definitive clinical trials evaluating this limiting intervention.
Five-year view
Most probably, the use of acetaminophen is going to decrease in the next few years from today's liberal use to a more limited one, but only when no other alternatives exist. Absolute banning does not seem possible or even adequate in the near future due to the lack of alternatives in some situations (newborns and infants below three months of age, intravenous use and ibuprofen contraindications such as ibuprofen intolerance and ibuprofen-associated serious gastrointestinal adverse events). This sharp decrease in population exposure to acetaminophen is likely to produce a measurable decrease in wheezing disorders prevalence and morbidity in childhood. "
- I clarified the text as per your request. Jytdog ( talk) 13:14, 24 February 2014 (UTC)
Nice work. Not to make light of a serious issue, but a very humorous take on correlation and causation here. Perhaps this image could be incorporated on the Monsanto page. http://www.pd.infn.it/~dorigo/autism_organic_foods.jpg Formerly 98 ( talk) 13:22, 24 February 2014 (UTC)
- laughing! But seriously, Martinez-Gimeno bases their thoughts on the epidemiologial evidence and this study, which they describe as follows:
To test the hypothesis that acetaminophen exposure increases wheezing disorders severity or morbidity in asthmatic children, and its corollary, that avoiding acetaminophen exposure in asthmatic children would improve asthma control and morbidity, a more attainable clinical trial design would be needed, recruiting asthmatic children (several substudies with different age limits) to be randomized to one of two arms: intervention versus no intervention (open-labeled) or acetaminophen versus ibuprofen (double-blind design). Again, a placebo arm, contrary to common claims, would be impractical and unethical. Primary outcome could be one of the many already used: days free of symptoms, symptoms scores, drug consumption scores, asthma exacerbations or asthma-related quality of life, and the duration necessary to obtain enough statistical power would be in the range of months, not years.
In fact, such a clinical trial already exists [15] . It was performed in the early 1990s but published in the early 2000s, when the hypothesis of the detrimental effect of acetaminophen in asthma had already been launched. Being the only clinical trial ever performed on the subject, it deserves careful reading and a detailed description. From 2 February 1991 to 12 June 1993, 84,192 children between 6 months and 12 years of age with a febrile illness were recruited and randomly assigned to receive suspensions of either acetaminophen (12 mg/kg) or ibuprofen (5 or 10 mg/kg) to test the safety profile of ibuprofen. A subgroup analysis of those children being treated for asthma, defined as those who had received a [beta]-agonist, theophylline (remember, we were in the early 1990) or an inhaled steroid on the day before enrollment, identified an outstanding number of 1879 children, 632 randomized to acetaminophen, 636 to ibuprofen low-dose and 611 to ibuprofen high-dose. Primary outcomes were a report of hospitalization or outpatient visit for asthma in the month after enrollment. The number of hospitalizations was too low to reach significance (eight, four and six in the acetaminophen, low-dose ibuprofen and high-dose ibuprofen groups, respectively), but the number of outpatient visits for asthma was higher in the acetaminophen group compared with both ibuprofen groups (5.0 vs 2.9%). The authors reported this difference computing an adjusted relative risk estimate using the Mantel-Haenszel procedure; adjusting for age, gender and race and considering the acetaminophen group as the reference category: this estimate was 0.56 (0.34-0.95) for ibuprofen. This estimate did not vary when multiple stratifications where performed and did not differ between both ibuprofen doses. It should be taken into account that this clinical trial was originally designed to test the hypothesis that among children with asthma and without a history of aspirin sensitivity, ibuprofen suspension for fever-control increased the risk of acute bronchospasm and other morbidities from asthma. However, they found exactly the contrary. In their paper, the authors did not mention the reason for the 11 years elapsed between the end of the clinical trial and its publication. The possibility exists that their results were so unexpected and so contrary to common beliefs at the time that they only decided to publish them when the whole acetaminophen detrimental effect of wheezing disorders hypothesis begun to arise. Even to date, this large and well-designed clinical trial is not receiving due attention and some authors continue to explain their results as a beneficial effect of ibuprofen instead of a detrimental effect of acetaminophen. As practicing pediatricians, this discussion is absolutely irrelevant: avoiding acetaminophen is absolutely equivalent to using ibuprofen, because no other alternative exists.
- which is pretty interesting. Jytdog ( talk) 13:32, 24 February 2014 (UTC)
- Yes, its one of the more persuasive papers. But it also highlights the multiple hypothesis testing problem that is so common in the medical literature, and which can be so frustrating to deal with since publication in peer-reviewed journals gives the conclusions of these papers so much legitimacy. Since they included both previously asthmatic and non-asthmatic children in the study, I presume that they looked for the possibility of increased asthma in both subgroups as well as the overall treatment population. They looked at both hospitalization and non-hospitalization ER visits as endpoints. So I'm counting at least 5 shots at a p<0.05 outcome already, and I don't know if they would have published if they had seen differences at specific timepoints, changes in medication use, etc. I find articles like this in which the pre-specified endpoints of the trial are not disclosed very frustrating, because they are tantilizing, yet in the final analysis uninterpretable.
Formerly 98 (
talk)
14:06, 24 February 2014 (UTC)
- i hear you! Jytdog ( talk) 14:17, 24 February 2014 (UTC)
- Yes, its one of the more persuasive papers. But it also highlights the multiple hypothesis testing problem that is so common in the medical literature, and which can be so frustrating to deal with since publication in peer-reviewed journals gives the conclusions of these papers so much legitimacy. Since they included both previously asthmatic and non-asthmatic children in the study, I presume that they looked for the possibility of increased asthma in both subgroups as well as the overall treatment population. They looked at both hospitalization and non-hospitalization ER visits as endpoints. So I'm counting at least 5 shots at a p<0.05 outcome already, and I don't know if they would have published if they had seen differences at specific timepoints, changes in medication use, etc. I find articles like this in which the pre-specified endpoints of the trial are not disclosed very frustrating, because they are tantilizing, yet in the final analysis uninterpretable.
Formerly 98 (
talk)
14:06, 24 February 2014 (UTC)
One of our key roles here on Wikipedia is to take complicated verbiage and get to the point.
This "A 1998 paper hypothesized that giving young children paracetamol may cause asthma later in life and while subsequent epidemiological studies have found a correlation between paracetamol use by young children and pregnant women and asthma, as of February 2014 it remained unclear if paracetamol actually has a role in causing asthma."
really means
"There is an association between paracetamol use and asthma but it is unclear if it has a role in causing asthma."
with the latter being much more clear and to the point. Thus restored. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 18:10, 24 February 2014 (UTC)
- I hear you on that! The key reason why I added the 1998 paper was in response to the question from Agyle above, where he wrote "What recommendations? Changed from what?" I thought those were valid questions.
Jytdog (
talk)
18:27, 24 February 2014 (UTC)
- Added the recommendation. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 19:02, 24 February 2014 (UTC)
- I hear you on that! The key reason why I added the 1998 paper was in response to the question from Agyle above, where he wrote "What recommendations? Changed from what?" I thought those were valid questions.
Jytdog (
talk)
18:27, 24 February 2014 (UTC)
- /* Simplier */
talk, thanks for reponse & quotes from Martinez-Gimeno. Sentence seems clearer now. However, this part, "but some experts have recommended that paracetamol use by children and pregnant women should be avoided.[48][49]", raises these issues about agreement between the cited sources and that part of sentence.:
- Martinez-Gimeno/García-Marcos [ref 48] (from the excerpt I read) recommends stopping “too liberal use” and “limiting its use to clinical situations in which no other alternatives remain” for all children. This does not mention pregnant women (perhaps it's mentioned elsewhere in the article, in which case disregard this; certainly use by pregnant women is questionable for non-asthma reasons). Also it's not saying to avoid its use in children entirely, including an exception for clinical situations with no alternatives. Since there are two authors, "some experts" is technically correct.
- McBride [ref 49] recommends “children with asthma or at risk for asthma should avoid the use of acetaminophen.” (Emphasis mine.) He does not mention pregnant women, or include healthy children, in that recommendation. I think his is a distinctly different recommendation from the one described in the Wikipedia article, and should be omitted as a source, or his view presented in addition to Martinez-Gemino's.
- Hope I'm not coming off as too nitpicky; your synthesis of all this feedback seems very good. :-) –– Agyle ( talk) 23:56, 24 February 2014 (UTC)
- /* Simplier */
talk, thanks for reponse & quotes from Martinez-Gimeno. Sentence seems clearer now. However, this part, "but some experts have recommended that paracetamol use by children and pregnant women should be avoided.[48][49]", raises these issues about agreement between the cited sources and that part of sentence.:
- not too nit-picky at all and your questions are all about making the article great. the original 1998 hypothesis was about infants and young kids. but as folks thought about the hyopthesis and designed epidemiologial studies, some of them took it back yet further. McBride (source 49, which is free) talks about this just a bit in ~3rd paragraph of the intro (search for "utero"). i would not be at all opposed to deleting the pregnancy thing (especially since it is secondary for even the most worried guy, McBride) - but in light of bobo's fierce concern about this issue, and since it didn't take a lot of space and wasn't inaccurate, i included it. but i am fine with it being deleted too. Jytdog ( talk) 01:10, 25 February 2014 (UTC)
- I didn't address your concern about the variation in "avoidance". in one of my first stabs at this, i think i set up three paths - change nothing; Martinez (which we agree on - use it only where you gotta), and Mcbride, which i framed as "stop using it". but you are right - it is "don't use it in kids with asthma or at risk for asthma." and you are right that nobody says boo about changig what pregnant women do. i just took that out. struggling with the other, especially in light of simplier. :) hmmm ok, made it "paracetamol should be given to children more selectively" - that covers both mcbride and martinez, yes? Jytdog ( talk) 01:25, 25 February 2014 (UTC)
- Restored Doc James version: Given "more selectively" seems vague.
- If you feel strongly about including "more selectively", I would not object to it being included along with a statement that experts have suggested avoidance, but not in place of it. Seems unbalanced and a downplay of the expert opinions.-- BoboMeowCat ( talk) 01:54, 25 February 2014 (UTC)
- "feeling strongly" has nothing to do with it. at this stage it is about trying to set up language that is good enough so we can all move on. i do think that argyle had a legit point about pregnancy, so i am taking that back out but will leave the "avoid" - that is 6 of one half a dozen of the other to me. Jytdog ( talk) 02:04, 25 February 2014 (UTC)
- The current text omits antipyretic use as an acceptable use by children ("...continue to recommend paracetamol for pain and discomfort in children....") I'd say “pain and fevers”, or something to that effect. Perhaps include discomfort too; AAP gives aches and soreness as examples, and Sullivan 2011 mentions improving comfort with regard to antipyretics. The cited EMA/HMA source seems more conservative than American recommendations (contrast AAP's casual examples to EMA/HMA's ”paracetamol should only be used during pregnancy or in children if clearly necessary”), but I can see ignoring this in the interest of simplicity.
- Regarding BoboMeowCat's “unbalanced and a downplay of the expert opinions”, I was actually thinking exactly the opposite. References [43]-[45] were all written/updated after [48] (Martinez-Gimeno/García-Marcos), and presumably considered their recommendation. Based on its current rejection by the scientific establishment, I'd suggest changing "some experts" to "a few experts", to better reflect its weight compared to the mainstream position(s), unless the recommendation comes from more than a single (though admittedly very strong) source.
- Agyle,I understand the nature of your assumption, but rejection not supported by references. Recommendations may represent maintenance of the status quo.-- BoboMeowCat ( talk) 04:14, 25 February 2014 (UTC)
- The UK National Institute of Clinical excellence updated their recommendations for treatment of fever in children in May 2013 and recommended treatment with either ibuprofen or acetominophen, with no preference stated. http://publications.nice.org.uk/feverish-illness-in-children-cg160/recommendations.
- In 2012, the World Health Organization developed recommendations for the treatment of chronic pain in children, recommending that mild pain be treated with acetominophen or ibuprofen. http://www.ncbi.nlm.nih.gov/books/NBK138340/
- The Italian Pediatric Association updated their guidelines in 2012 and also recommended ibuprofen or acetominophen. http://www.ncbi.nlm.nih.gov/pubmed/22742886?dopt=Abstract&holding=f1000,f1000m,isrctn
- Formerly 98 ( talk) 05:17, 25 February 2014 (UTC)
- BoboMeowCat, good point, cited sources don't indicate that the AAP or NHS considered any published reviews, let alone Martinez-Gimeno. We're still left, however, with medical organizations and most several recent reviews on one side, and a two-author review on the other. (McBride falls in the middle, but his view & recommendation are omitted from the current Wikipedia text.) I only just got access to Martinez-Gimeno, and noticed that in its section on other experts' opinions ("Experts' Opinion & Attitudes to the Acetaminophen as a Wheezing Disorders Promoter Hypothesis"), it cites four recently published reviews with status quo opinions, which it attributes to bias, and only McBride's suggesting any change in paracetamol usage. While it may well be correct, Martinez-Gimeno's review itself seems to make a case that it's a minority view among experts. Agyle ( talk) 06:13, 25 February 2014 (UTC)
- The NHS meticulously documents its search and deliberation procedures, and these can be found for the acetominophen recommendation, including the exact details of the adverse event search in the following document. http://guidance.nice.org.uk/CG/WaveR/108/HEPlanReviewQuestionsSearchStrategies/ReviewQuestionsSearchStrategies/pdf/English. The search strategy explicitly includes Medline and other database searches for adverse event related publications. (page 183).
- In their 2011 Fever treatment guideline, the AAP explicitly mentions the asthma hypothesis and states: "One safety concern is the effect of acetaminophen on asthma-related symptoms; although asthma has also been associated with acetaminophen use, causality has not been demonstrated." Having noted this association in 2011, it strains credulity to think they would not have considered it when they updated the guideline in 2013. http://pediatrics.aappublications.org/content/127/3/580.full
- I reverted your edit because I think it takes us back to where we were at the beginning of this 8,000 word argument: by expanding on the language for the minority position, it not only gives equal weight to the minority position, it actually emphasizes it. I just don't think you can counterpoint the opinion of NICE and the AAP with the opinion of 3 or 4 researchers. Its not balanced. Formerly 98 ( talk) 10:15, 25 February 2014 (UTC)
- The amount of time and effort we have put into these two sentences is like something out of a Monty Python skit. I'd like to propose that we hold a simple vote, choosing between the most recent version by Argyle and the prior version by Jytdog, and then put this to bed. Having just reverted Argyle, I'm obviously casting my vote for the Jytdog version. Formerly 98 ( talk) 10:26, 25 February 2014 (UTC)
- Formerly 98, I think you're misunderstanding things. I didn't change either sentence whatsoever, and it is not “my version”. Four days ago I did revert Bobo's change, but other than that, have not changed the section's text in any way. The edit you reverted were merely changes within the citations themselves, mostly touchups like capitalizing journal names and adding links to the text of the articles, but also including two quotes from the conclusions of the studies within the citations. (If you object to that, then remove just the "quote=" parts in the citations, and we can discuss it further). I'm reverting your reversion, under the good faith belief that you misinterpreted my edit.
- Per the suggestion to "just put this to bed", which you also suggested earlier, in a word: no. If there are improvements to be made, they should be made. Saying it's ok for children for pain and discomfort, but omitting its use as an antipyretic, deviates from almost all of the cited sources. It's minor, but I'm not letting it slide just because you want to be done with this. Agyle ( talk) 11:01, 25 February 2014 (UTC)
- No, I did mean to revert. Having additional arguments that flash up when you roll the cursor over the text does increase the weight given to the "stop all acetominophen use in children" POV, which was already too high. We're taking two papers and counterpoising them against the opinion of expert panels at the American Academy of Pediatrics and a review at the National Institute of Clinical Excellence. I don't think it makes sense.
- You joined this discussion at a point after which I had already spent many hours of work on it, and so my fatigue may not be something you relate to. I've had to defend myself against an unwarranted COI investigation and endless insinuations that I was engaging in shilling for a corporate client as well. Its fine to disagree that the 7408 words that have been spent on the topic here and the additional words over at COIN are not sufficient. But "I'm not letting it slide just because you want to be done with it" seems unnecessarily dismissive and disrespectful. I've put a lot of work into this, and while I do not expect others to always agree with me, it would be nice if they showed some respect for my efforts. Your efforts to fine tune the language are built on a foundation of many hours of work that I put in getting us away from language that you yourself have criticized as giving readers an incorrect impression.
- To avoid any misunderstanding, the "Monty Python" remark was a gibe at the process overall, including my own 5000 or so word contribution to the aforementioned 7400 words. It was not intended as a criticism of your work, and I apologize if I failed to make that clear. Formerly 98 ( talk) 14:01, 25 February 2014 (UTC)
- Agyle and Formerly 98, while I see the point regarding the recommendations for current continuation of status quo being more numerous than recommendations for avoidance, it seems that inclusion of statement regarding avoidance seems appropriate, particularly in light of fact that the earlier statement regarding "unclear" appears unbalanced. While certainly not proven beyond all doubt, there is abundant and varied evidence, which would provide additional clarity on the issue, yet has already been deleted:
- https://www.ncbi.nlm.nih.gov/pubmed/22065272
- https://www.ncbi.nlm.nih.gov/pubmed/15706003
- https://www.ncbi.nlm.nih.gov/pubmed/18805332
- https://www.ncbi.nlm.nih.gov/pubmed/18201589
- https://www.ncbi.nlm.nih.gov/pubmed/20205695
- https://www.ncbi.nlm.nih.gov/pubmed/20709817
- https://www.ncbi.nlm.nih.gov/pubmed/15735054
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1745727/
- https://www.ncbi.nlm.nih.gov/pubmed/19210907
- https://www.ncbi.nlm.nih.gov/pubmed/19210907
- https://www.ncbi.nlm.nih.gov/pubmed/18400839
- Including all of this abundant and varied evidence would make the section considerably more lengthy, and in terms of briefly, the current statement regarding avoidance seems to provide some of the missing balance for all of the above mentioned omitted content.-- BoboMeowCat ( talk) 16:42, 25 February 2014 (UTC)
User:BoboMeowCat. The causal link is not proven; not a single source that you bring above says that it is. It is also a fact, as the article states, that the mainstream view has not yet shifted to changing acetaminophen administration to kids based on a concern about this. This is how wikipedia works; we give the WP:WEIGHT to the mainstream, consensus view, which we identify through the statements of major medical bodies, as we have done here. We represent, but give less weight to, minority views, which we have also done here. Wikipedia is not here to WP:RIGHTGREATWRONGS - we give the weight to the mainstream, consensus views. If you want to advocate for changing the mainstream view, Wikipedia is not the place to do it. Please read WP:ADVOCACY. When a mainstream medical body changes its recommendation based on a concern about asthma, we can revisit this. If you know of any that have done so, please bring a source for that. Until you do, the article is going as far as it can. I am giving you a heads up here now - I and others have explained, based on Wikipedia guidelines and policies, ( WP:MEDRS and WP:WEIGHT) how the content you are interested in is handled at Wikipedia. Further, no one is supporting your position that the mainstream says that acetaminophen causes asthma nor a position that the minority view deserves more weight. Please read WP:IDHT - you are getting pretty close to falling squarely within that. I for one am going to stop responding to you pretty soon, until you bring the kind of sources we need to go further. You are new here, so I am trying to warn you very clearly. If you continue to try to actually edit the article to increase the weight given to this issue, without bringing the kind of source needed to give it more weight, I'll bring you to the WP:NPOVN board, and you will get blocked again or perhaps even topic banned. I hope you do not go in that direction, but based on your behavior thus far (blocked for editing warring, then bringing a groundless COIN case, and coming back here and repeating yourself) my guess is that you are are not going to listen. I hope you do listen. best regards Jytdog ( talk) 18:06, 25 February 2014 (UTC)
- There seems to be misrepresentations present in the above comment. If you review my edits and talk history, it shows I've never stated it was proven that paracetamol causes asthma. I have not advocated policy change. However, I have objected to the repeated deletion of accurate and properly sourced content (which at this time remains deleted) because that seems unbalanced/not neutral. Specifically, this content includes factors which provide clarity regarding the epidemiological link to asthma. As this discussion has become very lengthy, I'll repeat factors:
- (1) a dose-response relationship between paracetamol use and asthma;
- (2) the results of a double blind trial comparing paracetamol to ibuprofen for treatment of fever in asthmatic children;
- (3) the strength of the association between paracetamol use and asthma;
- (4) the consistency of this association across different geographical areas and different cultures;
- (5) the timing of increased paracetamol use in relation to the asthma epidemic
- (6) a relationship between per-capita sales of paracetamol and asthma prevalence across multiple countries;
- (7) the association between use of paracetamol by mother during pregnancy and increased wheezing in early childhood; and
- (8) a biologically plausible mechanism of glutathione depletion in airway mucosa.
- These factors were referenced by the above linked 11 peer reviewed medical journal articles (which included both primary and secondary sources) yet it was deleted. Also please note, I have not reinstated this deleted content, but rather objected to the deletion of additional content, because that additional deletion, on top of the already significant deletion, would seem to further reduce balance/neutrality.-- BoboMeowCat ( talk) 18:57, 25 February 2014 (UTC)
- ok, please pardon me that i missed the emphasis. please do stop repeating yourself. again (and it is the last time I will address this), i point you to WP:WEIGHT, which is policy, and which you are ignoring. The article is very clear and unambiguous that p. use and later asthma are correlated. the points you keep bringing are the criteria that are used to argue for causation. as others have already written to you, as of the date we are writing, the mainstream view is that causation is not established and that the recommendations are unchanged. As per WP:WEIGHT, we do not give more weight to the minority view which is that causation is established. now, the mainstream view may evolve. if and when it does, we can update the article. again, please let this go already and please stop repeating yourself. the WP article has gone as far as it can on the point you care about, which at this time is not the mainstream view. the only sources that will be compelling for this, will be a change in a statement by one of the major medical bodies that we cite, or a new statement by one we don't cite yet. thanks. Jytdog ( talk) 19:26, 25 February 2014 (UTC)
I can live with the wording of the most recent revision by BoboMeowCat. If he is satisfied, we may be close to consensus. Formerly 98 ( talk) 20:37, 25 February 2014 (UTC)
- Today's statement switched back to McBride's recommendation, and is now listing only the AAP and NICE as competing views. The approach seems designed to diminish the mainstream view, but I'm not sure how that can be countered with the requirement of proving a guideline is current as of 2014, except in the cases (like AAP & NICE) where they're repeated on layperson-friendly websites which are presumed to be current. Consider the WHO or JPS, for example, who also published recommendations for paracetamol use by children without any mention of asthma or risk of asthma. WHO publishes recommendations in rarely-released books, with periodic updates in the interim, so their most recent recommendations (I think, but can't prove) are from 2005. Similar issue with the JPS's 2012 guidelines. Are we omitting them because they don't have a dumbed down website?
- Handbook: IMCI Integrated Management of Childhood Illness (PDF). World Health Organization. 2005. pp. 47, 49–50, 55, 88, 92, 97, 102, 112, 145. ISBN 92 4 154644 1.
- Ishizaki, Yuko; et al. (2012). "Japanese clinical guidelines for chronic pain in children and adolescents" (PDF). Pediatrics International. 54 (1). Japan Pediatric Society: 1–7. doi: 10.1111/j.1442-200X.2011.03543.x. ISSN 1328-8067.
- The National Health Service does have a ”consumer“ website, and I think can be added uncontroversially:
- "Painkillers, paracetamol". NHS Choices. UK National Health Service.
- I guess the reason I'm content with it is that I consider both NICE ande AAP to be the most authoritative sources by far among those listed. I may be overestimating the extent to which others will see it the way I do, but I'm getting less demanding as time goes on out of sheer exhaustion. Formerly 98 ( talk) 03:02, 26 February 2014 (UTC)
Acetaminophen & asthma
Have added that "The majority of the evidence does not; however, support a causal role." for acetaminophen based on "The weight of evidence of the collected studies in our review strongly suggests that the association of antibiotics with childhood asthma reflects various forms of bias, the most prominent of which is confounding by indication. Recent studies and meta-analyses support the same conclusion for paracetamol. " [4] Doc James ( talk · contribs · email) (if I write on your page reply on mine) 14:32, 18 May 2014 (UTC)
- You are confusing "antibiotics" with "acetaminiophen". See your edit summary over on asthma article. Additionally, the most recent studies would reflex primary research. Secondary research of multiple studies only supports this claim for antibiotics --
BoboMeowCat (
talk)
14:40, 18 May 2014 (UTC)
- Not by my reading. Doc James ( talk · contribs · email) (if I write on your page reply on mine) 14:53, 18 May 2014 (UTC)
- You are confusing "antibiotics" with "acetaminiophen". See your edit summary over on asthma article. Additionally, the most recent studies would reflex primary research. Secondary research of multiple studies only supports this claim for antibiotics --
BoboMeowCat (
talk)
14:40, 18 May 2014 (UTC)
- BoboMeowCat can you not see that the abstract says "Recent studies and meta-analyses support the same conclusion for paracetamol."? Jytdog ( talk) 16:40, 18 May 2014 (UTC)
- Recent edit written by Jytdog and restored by DocJames not supported by the references. https://en.wikipedia.org/?title=Paracetamol&oldid=609098410
- Here’s the edit:
- “There is an association between paracetamol use and asthma but the weight of evidence of the collected studies strongly suggests that the association reflects various forms of bias, the most prominent of which is confounding by indication.[46] The majority of the evidence does not support a causal role.[47]”
- To break it down, the first part: “the weight of evidence of the collected studies strongly suggests that the association reflects various forms of bias, the most prominent of which is confounding by indication”
- It’s referenced by this source. https://www.ncbi.nlm.nih.gov/pubmed/23347656 From article abstract:
- “There is substantial epidemiological evidence in adults and children that acetaminophen use is associated with asthma symptoms. There is also a considerable body of evidence that supports a modest but consistent association of acetaminophen use in pregnancy and early infancy with asthma in later childhood. This relationship is robust to adjustment for a large range of potential confounding factors and, in some studies, shows clear evidence of a dose-dependent association but the possibility of confounding by indication has remained a concern. However, the epidemiological evidence is now compelling and there is a clear need to establish causation so that appropriate advice and interventions can be developed for children at risk of asthma. This requires randomised trials of analgesics and antipyretics, including acetaminophen, in a variety of clinical settings.”
- I'm confused how “the weight of evidence of the collected studies strongly suggests that the association reflects various forms of bias, the most prominent of which is confounding by indication”, could be concluded from this article. This article did not say the weight of the evidence suggests bias, but rather the article left bias open as a possibility. At best this seems an example of extreme WP:Cherrypicking
- The second part, “The majority of the evidence does not support a causal role” is referenced by this article https://www.ncbi.nlm.nih.gov/pubmed/23292157. The discussion section of this article says the majority of evidence does not support a causal role for antibiotics and recent studies suggest “confounding of indication” for acetaminiophen. Recent studies does not equal the majority of studies.
- If you look at the above 2 secondary sources on asthma and acetaminophen/paracetamol along with these additional secondary sources:
- It seems clear that the previous edit is does not reflect the data on the topic of paracetamol and asthma neutrally and accurately.--
BoboMeowCat (
talk)
03:45, 20 May 2014 (UTC)
- The ref says "Recent studies and meta-analyses support the same conclusion for paracetamol." It is from 2013 which is newer than 2011.
Doc James (
talk ·
contribs ·
email) (if I write on your page reply on mine)
09:22, 20 May 2014 (UTC)
- That’s referring to confounding of indication. Recent studies suggest confounding of indication may be issue with paracetamol/acetaminophen, which was reflected in my version of the edit. Also, newer doesn’t prove better, if it did, we would not have the WP:MEDRS restriction regarding primary research, which tends to be the newest research. Recent studies cannot logically reflect the majority of the evidence. Please stop restoring content not supported by the references cited.--
BoboMeowCat (
talk)
11:12, 20 May 2014 (UTC)
- Do you know what "confounding by indication" refers to? Doc James ( talk · contribs · email) (if I write on your page reply on mine) 11:29, 20 May 2014 (UTC)
- That’s referring to confounding of indication. Recent studies suggest confounding of indication may be issue with paracetamol/acetaminophen, which was reflected in my version of the edit. Also, newer doesn’t prove better, if it did, we would not have the WP:MEDRS restriction regarding primary research, which tends to be the newest research. Recent studies cannot logically reflect the majority of the evidence. Please stop restoring content not supported by the references cited.--
BoboMeowCat (
talk)
11:12, 20 May 2014 (UTC)
- The ref says "Recent studies and meta-analyses support the same conclusion for paracetamol." It is from 2013 which is newer than 2011.
Doc James (
talk ·
contribs ·
email) (if I write on your page reply on mine)
09:22, 20 May 2014 (UTC)
- It seems clear that the previous edit is does not reflect the data on the topic of paracetamol and asthma neutrally and accurately.--
BoboMeowCat (
talk)
03:45, 20 May 2014 (UTC)
- I'd suggest that the article should reflect the "average" of the last half dozen or so secondary references and not give outsized weight to the most recent one. But having said that, I have not dug into this issue again to an extent that allows me to say whether this is already the case in the version proposed by DocJames.
- With regard to the language BobMeowCat is promoting, from my POV this absolutely does not fly. Four or five editors engaged with him on the issue of the McBride review for literally thousands of words of debate just a month or two ago. The overwhelming consensus of this group was that extensively quoting the one review out of a dozen that argued for a causative relationship was undue weight. In my opinion, his current attempt to bring this back in again after a clear expression of consensus against it is just plain disruptive editing, and takes this discussion outside the realm of a mere content dispute into a violation of the behavioral guidelines. This may need to be taken up on the Admin notice board if it continues. Formerly 98 ( talk) 13:21, 20 May 2014 (UTC)
Acetaminophen Reduces Both Pain and Pleasure, Study Finds
- Thanks but we only use secondary sources generally.
Doc James (
talk ·
contribs ·
email)
07:36, 14 April 2015 (UTC)
- Original Ohio State University article handle embargoed from February last year, and the DOI for the published article in PSS. Jon ( talk) 10:14, 14 April 2015 (UTC)
- Thanks but we only use secondary sources generally.
Doc James (
talk ·
contribs ·
email)
07:36, 14 April 2015 (UTC)
Well, I added a brief entry under "Adverse Effects" with a reference. I'm not convinced it's a necessarily adverse effect, but certainly interesting :-) I used the new in-place editor to add the reference; not sure how to add multiple authors; shall amend presently with the markup editor. Jon ( talk) 10:33, 14 April 2015 (UTC)
- nether source is OK for health related content - the scientific article is a PRIMARY source (please see Wikipedia:Identifying_reliable_sources_(medicine)#Definitions) and also please see Wikipedia:Identifying_reliable_sources_(medicine)#Respect_secondary_sources, specifically about the popular media source hyping the PRIMARY source. We need to wait until this is discussed in SECONDARY source (see definitions above). Someone else already reverted the addition on these grounds.. hope that makes sense. Jytdog ( talk) 12:17, 14 April 2015 (UTC)
- I see! Fair enough so. I thought you were talking about TERTIARY sources. Jon ( talk) 13:24, 14 April 2015 (UTC)
Hyperactivity and Neural Development - Censorship
Two recent studies indicate problems in hyperactivity [1] and neural development [2] of children.
- Yeah, so I add two interesting and important new, relevant references to an article which indicates potential harm to pregnant women on the Paracetamol page. These are removed because you guys don't like primary sources? This is ridiculous and frankly an extreme case of what is wrong with Wikipedia. My wife is pregnant. I for sure want to know about potential harm of this drug. I would think as a medical professional that you would be more inspired by the "first do no harm" idea. The fact that you Wikipedia jerks are so focused on having only sources from a narrow range of whatever it takes for a given article is so frustrating. I've continued to run into this kind of thing. You would think that academic journals have taken over Wikipedia. The idea that I have actually improved the article with my additions, and that others can improve it further, has completely escaped much of the Wikipedia culture these days. Wikipedia has simply forgotten the idea that this is collaboratively edited, rather than having a coterie of people who simply reject all edits if they do not thread the eye of the needle through the dozens of acronym style guides. You guys are disgusting, really. You are standing on the shoulders of millions of edits and now you reject the very thing that got you to where you are, namely lots of collaboratively edited small improvements. Now any change has to go through hurdles that would never have created Wikipedia in the first place. The fact that you have excluded something that is evidence of significant danger to pregnant women based on this culture of exclusiveness should trouble you deeply. -- Jeffmcneill ( talk) 03:01, 27 July 2015 (UTC)
References
- ^ Liew Z, Ritz B, Rebordosa C, Lee PC, Olsen J (2014). "Acetaminophen use during pregnancy, behavioral problems, and hyperkinetic disorders". JAMA Pediatr. 168 (4): 313–20. doi: 10.1001/jamapediatrics.2013.4914. PMID 24566677.
- ^ Brandlistuen RE, Ystrom E, Nulman I, Koren G, Nordeng H (2013). "Prenatal paracetamol exposure and child neurodevelopment: a sibling-controlled cohort study". Int J Epidemiol. 42 (6): 1702–13. doi: 10.1093/ije/dyt183. PMC 3887567. PMID 24163279.
New potential source
This looks like a good source:
Should you take Tylenol, Advil, or aspirin for pain? Here's what the evidence says. (vox.com)
-- Distelfinck ( talk) 22:17, 18 August 2015 (UTC)
- That source doesn't meet WP:MEDRS, but thanks for bringing it. Jytdog ( talk) 10:41, 19 August 2015 (UTC)
- Alright. There's lots of links to scientific articles in it though, so we could use those as sources -- Distelfinck ( talk) 14:12, 19 August 2015 (UTC)
- We already comment on the issue of back pain using the high quality sources
[5]
Doc James (
talk ·
contribs ·
email)
15:32, 19 August 2015 (UTC)
- Distelfinck please do read WP:MEDRS and per Doc James the content in the article is already supported by the sources that meet MEDRS well. Jytdog ( talk) 15:39, 19 August 2015 (UTC)
External links modified
Hello fellow Wikipedians,
I have just added archive links to one external link on
Paracetamol. Please take a moment to review
my edit. If necessary, add {{
cbignore}} after the link to keep me from modifying it. Alternatively, you can add {{
nobots|deny=InternetArchiveBot}} to keep me off the page altogether. I made the following changes:
- Added archive https://web.archive.org/20130912075213/http://www.nhs.uk:80/Conditions/Flu/Pages/selectorshow.aspx?medicine=Phenylephrine/Guaifenesin/Paracetamol to http://www.nhs.uk/Conditions/Flu/Pages/selectorshow.aspx?medicine=Phenylephrine/Guaifenesin/Paracetamol
When you have finished reviewing my changes, please set the checked parameter below to true to let others know.
This message was posted before February 2018.
After February 2018, "External links modified" talk page sections are no longer generated or monitored by InternetArchiveBot. No special action is required regarding these talk page notices, other than
regular verification using the archive tool instructions below. Editors
have permission to delete these "External links modified" talk page sections if they want to de-clutter talk pages, but see the
RfC before doing mass systematic removals. This message is updated dynamically through the template {{
source check}} (last update: 5 June 2024).
- If you have discovered URLs which were erroneously considered dead by the bot, you can report them with this tool.
- If you found an error with any archives or the URLs themselves, you can fix them with this tool.
Cheers.— cyberbot II Talk to my owner:Online 16:32, 6 February 2016 (UTC)
More research needed
I am not a big fan of this bland statement as this is true for half the stuff in Wikipedia. Therefore have removed "however, further studies are needed to evaluate the validity of concerns regarding the neurological development of the offspring" Doc James ( talk · contribs · email) 09:32, 12 July 2016 (UTC)
- In this case it looks more like your opinion prevails over the conclusion of the authors.
[6]
Ekem (
talk)
17:43, 12 July 2016 (UTC)
- Not at all. User:Doc James is precisely reflecting the cited article, which says essentially "of course, our study isn't definitive (very few are), but as far as we can tell, XXX". I agree completely with Doc James's edit. -- Macrakis ( talk) 02:29, 13 July 2016 (UTC)
- Further studies, such as this? "Prenatal exposure to acetaminophen and children's language development at 30 months." [1]
Toxicity
User:Abductive your changes here and here and here are adding WP:UNDUE weight to the risks of this drug, and the content you added about "physicians have not internalized these results and continue to recommend" is unsupported editorializing. If you add this back one more time you will violate 3RR and can be blocked. Jytdog ( talk) 18:16, 16 August 2016 (UTC)
- Really? You sure are quick to dismiss the edits. Perhaps you should ask for more citations instead?
Abductive (
reasoning)
18:17, 16 August 2016 (UTC)
- This subject has been extensively discussed here on Talk. See
here and the section below that and elsewhere. The existing content is the result of careful discussion and accurately reflects the sources.
Jytdog (
talk)
18:18, 16 August 2016 (UTC)
- All you are doing is reverting, denying scientific source I added to the article. You need to read the source.
Abductive (
reasoning)
18:30, 16 August 2016 (UTC)
- In the third dif above you removed a very strong source, PMID 25851072 - a review from 2015 - and added a weak source - a hot off the presses primary source here that the field has not even had time to consider yet. This is not how we edit about medicine. See WP:MEDRS, particularly the WP:MEDREV section. Jytdog ( talk) 18:55, 16 August 2016 (UTC)
- You have now reverted a fourth time. I won't follow you over that line. Jytdog ( talk) 19:10, 16 August 2016 (UTC)
- All you are doing is reverting, denying scientific source I added to the article. You need to read the source.
Abductive (
reasoning)
18:30, 16 August 2016 (UTC)
- This subject has been extensively discussed here on Talk. See
here and the section below that and elsewhere. The existing content is the result of careful discussion and accurately reflects the sources.
Jytdog (
talk)
18:18, 16 August 2016 (UTC)
Paracetamol is generally accepted as safe during pregnancy as supported by the references provided. One of the articles does not appear to be pubmed indexed [7]? Doc James ( talk · contribs · email) 19:17, 16 August 2016 (UTC)
- Yes too new to be indexed yet! Jytdog ( talk) 20:22, 16 August 2016 (UTC)
- Just to note
there's a more recent review on the matter from last December which essentially echos the current text.
M. A. Bruhn (
talk)
21:05, 16 August 2016 (UTC)
- There's also a somewhat more recent review which states "the literature examined in this article suggests a review of the widespread opinion that acetaminophen is safe during pregnancy". I believe it might be a good time to revisit the current text in the article and make some slight alterations. M. A. Bruhn ( talk) 21:23, 16 August 2016 (UTC)
FYI this has appeared in the uk press today. - Roxy the dog™ bark 21:29, 16 August 2016 (UTC)
- When that primary study appears in a review, we can cover it. However, I'd note that the conclusion of the paper doesn't establish causality. It just points out that there is evidence against confounding factors involved in the correlation. In reality, the relationship could be causal - this isn't implausible since paracetamol's biomolecular targets are expressed in brain cells - however this has not been established yet in any research. It's important not to overstate the facts since it's also possible that there are other confounding factors (see omitted variable bias) that are unrelated to mid-/post-pregnancy paracetamol use and partner paracetamol use. Seppi333 ( Insert 2¢) 19:34, 17 August 2016 (UTC)
Article on Acetaminophen and Behavioural disorders
A very large study suggesting that Acetaminophen or Paracetamol use doing pregnancy may be responsible for ADHD and other disorders in childrem
http://www.ncbi.nlm.nih.gov/pubmed/24566677Cite error: There are <ref> tags on this page without content in them (see the
help page).
This should be part of the discussion on this drug. 2602:306:BCED:1070:6809:6C22:4C3:FD07 ( talk) 17:41, 22 August 2016 (UTC)
- 2 year old study that has been discussed to death here. Jytdog ( talk) 17:45, 22 August 2016 (UTC)
Requested move 16 November 2016
- The following is a closed discussion of a requested move. Please do not modify it. Subsequent comments should be made in a new section on the talk page. Editors desiring to contest the closing decision should consider a move review. No further edits should be made to this section.
The result of the move request was: Not moved per WP:SNOW. ( non-admin closure) Zarcadia ( talk) 20:50, 16 November 2016 (UTC)
Paracetamol →
Para-acetylaminophenol –
WP:COMMONALITY ; this should not favour either British English (paracetamol) or North American English (acetaminophen), instead it should use the origin term that paracetamol (para-acetylaminophenol) and acetaminophen (para-acetylaminophenol) and Tylenol (para-acetylaminophenol) are abbreviations of, namely "
para-acetylaminophenol" --
65.94.171.217 (
talk)
04:30, 16 November 2016 (UTC)
Survey
- Feel free to state your position on the renaming proposal by beginning a new line in this section with
*'''Support'''or*'''Oppose''', then sign your comment with~~~~. Since polling is not a substitute for discussion, please explain your reasons, taking into account Wikipedia's policy on article titles.
- Support I am the nominator; no biases in the dialect used, and "P-acetylaminophenol" is not too uncommon either. -- 65.94.171.217 ( talk) 04:32, 16 November 2016 (UTC)
- Oppose not even close to WP:COMMONNAME. Not in popular use nor in the literature. This will be a snow close. Jytdog ( talk) 05:01, 16 November 2016 (UTC)
- Oppose as Jytdog In ictu oculi ( talk) 07:47, 16 November 2016 (UTC)
- Oppose, totally inappropriate suggestion, please close per WP:SNOW. MrStoofer ( talk) 09:33, 16 November 2016 (UTC)
- Snowpose. Paracetamol is not limited to British English, but is actually the international nonproprietary name and far more common than this chemical monstrosity. -- HyperGaruda ( talk) 18:26, 16 November 2016 (UTC)
Discussion
- Any additional comments:
- The above discussion is preserved as an archive of a requested move. Please do not modify it. Subsequent comments should be made in a new section on this talk page or in a move review. No further edits should be made to this section.
INN
What is the INN of paracetamol? - DePiep ( talk) 21:57, 25 November 2016 (UTC)
- I think it is paracetamol. Doc James ( talk · contribs · email) 23:53, 25 November 2016 (UTC)
Cochrane blog
User:Jtamad why are you adding a blog source to a medical section? Jytdog ( talk) 03:57, 19 August 2017 (UTC)
References
- ^ Bornehag, C.-G.; Reichenberg, A.; Hallerback, M. Unenge; Wikstrom, S.; Koch, H.M.; Jonsson, B.A.; Swan, S.H. "Prenatal exposure to acetaminophen and children's language development at 30 months". European Psychiatry. doi: 10.1016/j.eurpsy.2017.10.007.
Effectiveness in children
There is a blanket statement at the start of this article which seems to be entirely out of place and largely false.
"There is poor evidence for fever relief in children."
This links to a meta-study that is 15 years old, that contains a very small sample size.
Even as somebody who is not medical, this statement seems absurd, given that many people have success with paracetamol for fever relief in children. Even my local world renowned children's hospital (Royal Children's Hospital in Melbourne, Australia) have guidelines written in 2013 that recommend the use of paracetamol for fever relief.
http://www.rch.org.au/kidsinfo/fact_sheets/Pain_relief_for_children_-_Paracetamol_and_Ibuprofen/
I would think it prudent to just remove this sentence altogether, as it is totally out of place and at odds with common sense. — Preceding unsigned comment added by Jessejackson100 ( talk • contribs) 02:49, 27 May 2017 (UTC)
Jessejackson100 ( talk) 02:56, 27 May 2017 (UTC) JJ
- I doubt much has changed since 2002. Do you have a source that says their is good evidence? Temps go up and they come down, thus one needs a placebo controlled trial. Doc James ( talk · contribs · email) 03:38, 27 May 2017 (UTC)
- But you understand what I'm saying here? The tone of that sentence is such that a casual reader would take it to mean that paracetamol 100% does not work in children. At least that's what I hear when I see the words "poor evidence". I am a sample size of 1, but I have seen it 100% work in a child on multiple occasions. This sentence as it is currently structured doesn't seem to allow for the fact that in some circumstances, it works. This Wikipedia article is the first I've ever heard of this, which is contrary to the advice I've been given by every medical doctor I've been in contact with on every occassion that I've had a sick child with a fever.
- A search on Google scholar for articles relating to fever management in children brings up a number of more recent articles, many which are comparing paracetamol to ibuprofen in children. They all seem to agree that ibuprofen is more effective, but none of them state that paracetamol plain doesn't work. It appears that there are limited studies though in this field, and that single meta study with n = 1500ish doesn't seem to warrant the finality of this statement.
Jessejackson100 (
talk)
10:29, 27 May 2017 (UTC)
- I have seen doing nothing work frequently as well. Indeed ibuprofen appears to work better than acetaminophen. The question is does acetaminophen work better than placebo?
- Basically we need properly done RCTs with the comparison being placebo to show whether or not paracetamol works. The little evidence there is says it does not.
Doc James (
talk ·
contribs ·
email)
17:26, 27 May 2017 (UTC)
- I just did a mini review of the literature and I don't see many new RCTs on this topic. I was initially a bit puzzled why I didn't see Cochrane publish an updated review but I suppose it wouldn't be very meaningful since it would likely just reiterate the findings from the 2002 review since there isn't much new data. TylerDurden8823 ( talk) 18:01, 28 October 2017 (UTC)
- A search on Google scholar for articles relating to fever management in children brings up a number of more recent articles, many which are comparing paracetamol to ibuprofen in children. They all seem to agree that ibuprofen is more effective, but none of them state that paracetamol plain doesn't work. It appears that there are limited studies though in this field, and that single meta study with n = 1500ish doesn't seem to warrant the finality of this statement.
Jessejackson100 (
talk)
10:29, 27 May 2017 (UTC)
Effectiveness
The article seems very weak on evidence that paracetamol really has any pain-relieving effect at all. Largely the article just seems to take it for granted that it does actually work, with the exception of a couple of special applications where efficacy is questioned. For me the effect of paracetamol on any type of pain (that I have tested) is zero to undetectable. I know that I am not unique in this respect. 86.191.44.105 ( talk) 04:31, 2 February 2017 (UTC)
- There is evidence for some stuff. But yes it is a weak pain medication. Doc James ( talk · contribs · email) 05:54, 2 February 2017 (UTC)
- Agreed, it's a low-strength analgesic. TylerDurden8823 ( talk) 18:02, 28 October 2017 (UTC)