| This is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 | Archive 2 | Archive 3 | Archive 4 | Archive 5 | Archive 6 | → | Archive 10 |
DO NOT EDIT OR POST REPLIES TO THIS PAGE. THIS PAGE IS AN ARCHIVE.
This archive page covers approximately the dates between 20 May, 2005 and 20 June, 2005
Post replies to the main talk page, copying or summarizing the section you are replying to if necessary.
New Images
I've added two images from the National Institute of Health. The first--"HIV Viron.png"--replaces the old "Aids virus.jpg" image. The new image is clearer and provides a better description of the anatomy of the HIV viron. The second image--"HIV Daughter Particles.jpg"--illustrates the text about replication of HIV after and initial infection (under the "Current medical understanding of AIDS" section).
Please be nice to the new images while waging revert wars... Carl Henderson 04:26, 4 Jun 2005 (UTC)
fred's edit
I have removed. "During situations where treatments are available many people are able to delay death between ten to twenty years after the development of AIDS." becuase there is no factual basis for this claim. Show me the reference to a ten year survival for antiretrovirals . if you want to make this claim.
Also I have added. "In a process still imperfectly understood, HIV infects the CD4 cells (also called T4 or T-helper cells) of the immune system" This is the current 2005 "scientific consesus". Fauci of NIH from memory.
I have a problem with "AIDS typically develops about ten years following HIV infection." I think ten years is probably the 50% survival - so half develop AIDS within 10 tears and after 10 years half have not developed AIDS. Calling a mid point of a range "typical" seems misleading as in fact very few people wil actually develop AIDS in years 10
Also "proper administration" of antiretroviral medicatiom, seems unnecesarily contentious. Is there evidence of improper adminstration - is it itended to suggest that all or some doctors are imcompetent?
Fred2005 14:49, 11 Jun 2005 (UTC)
Symptoms
I have a problem with this:
- HIV is transmitted by bodily fluids, such as blood, semen, breast milk, and vaginal secretions. It causes disease by infecting CD4+ T cells, a type of leukocyte (white blood cell) that normally coordinates the immune response to infection and cancer. When a person's CD4+ T cell count decreases sufficiently he or she is prone to a range of diseases that a healthy person's body is normally able to fight. These diseases include cancers and opportunistic infections, which are usually the cause of death in persons with AIDS. HIV may also infect brain cells, causing some neurological disorders.
How is this relevant to Symptoms of AIDS?
The whole issue is that the first symptom of AIDS is usually an AIDS defining illness. Two thirds of reported AIDS in the United States is on the basis of low CD4 cell count - these cases are all asymptomatic
Also opportunistic infections was replaced by AIDS defining illness back in 1993. Can we move with the times and keep up to date with the scientific consenus please?
If you read the Pneumocystis jiroveci pneumonia article you will see that we have all moved on from the earlier suggestions about opportunistic infections. Fred2005 16:00, 11 Jun 2005 (UTC)
Prevention
Deleted "There is now some evidence that treatment of already-infected people with antiretroviral drugs may reduce the transmission of HIV infection to their sexual partners, independently of other safer-sex precautions [9] ( http://en.wikipedia.org/wiki/AIDS#endnote_BBCHAARTspread). This may imply that aggressively treating existing HIV cases, in addition to protecting the uninfected population through education and safer-sex programs, may be more effective at preventing the spread of HIV that either of these alone."
The scientific consesus is that people on retrovirals should use condoms, even if their viral load is undetectable Joe Merkel 02:23, 12 Jun 2005 (UTC)
- I'm uncertain on how well-supported the evidence is on this point, but in general I think you're seeing a contradiction where none needs to exist. Even if the risk of transmission is reduced by treatment, it doesn't mean that you still wouldn't advise the use of condoms to reduce the risk further. So unless the evidence for this reduced transmission is marginal in and of itself, I think the appropriate action would be to reinstate the sentence and note that this doesn't make it wise for HIV-positive people to have unprotected sex. -- Robert Merkel 07:43, 12 Jun 2005 (UTC) (no relation)
- I agree with you that we cannot determine from the linked newspaper article how well-supported the evidence is on this point. But the treatment guidelines have changed so much since 1997 that this research is largly irrelevant. The hit hard, hit early glory days are gone, because the scientific consenus has accepted the many studies showing unnacceptably high drug toxicity. Joe Merkel 15:38, 12 Jun 2005 (UTC)
- Hmmm. For one thing, the study began in 1997; given that it was published in 2004 I would suggest that the data would go to at least 2002. Seconldy, the latest source Sci Guy has dragged up suggests that treatment with low viral loads and high CD4+ counts is recommended against, but it says that for people with high viral loads that whether to offer treatment is controversial, particularly when the CD4+ counts are above 350/mm3. So , on the basis of that link (and it appears to be current and from a relevant, reputable source) the science isn't settled on exactly when to start treatment, and there seems to be some consideration for treatment purely to reduce viral loads. -- Robert Merkel 07:13, 13 Jun 2005 (UTC)
- That is correct, Robert. Treatment purely to reduce viral loads in people who have not been diagnosed with AIDS is now considered controversial in the United States. This is a big change in direction since the 1997 treatment guidelines. I am happy to read your Taiwanese research if you have a reference. The BBC article did not name an author. Sci guy 13:50, 13 Jun 2005 (UTC)
- I think you're reading more into the description of "controversial" than you should. I suspect "controversial" in this context means that the evidence that treatment is beneficial is unclear, and therefore some substantial group of clinicians think it's worthwhile and others don't. The jury is still out. Have a look at some of the criteria on which the decision to treat might be based, though; it includes likelihood of compliance with treatment. I suspect there might be more to it than drug toxicity; treatment, particularly imperfectly-applied treatment, might promote drug resistance and reduce treatment options later. -- Robert Merkel 23:53, 13 Jun 2005 (UTC)
- No Robert, this is the jury report. Controversial means the jury considered the evidence and does not recommend treatment. This is your scientific consenus in action. Facts change the minds of scientists, juries and politicians. Sci guy 03:26, 14 Jun 2005 (UTC)
- That's not what the text indicates. If there were a scientific consensus that treatment was not indicated, that guide wouldn't use the world "controversial". Looks like it might be time to dig up more information...-- Robert Merkel 03:43, 14 Jun 2005 (UTC)
- "Controversial" is a highly charged word. We should simply report facts. The optimum time to begin therapy remains an unresolved issue. It is recognized that therapy should begin before there is an irreversible deterioration of the immune system, and recommendations have varied: in 1987, treatment was delayed until patients had developed clinical AIDS; in 1996, the "hit-early-hit-hard" premise prevailed, and patients were treated when their CD4 count was <500/cmL. The current recommendations call for an intermediate approach: patients with CD4 counts < 200 should be treated, patients with CD4 counts > 350 who are asymptomatic should not be, and the decision on when to initiate treatment for patients with CD4 counts between 200 and 350 is based on rate of CD4+ cell count decline, HIV load (>100,000 copies is the number for concern), pregnancy, and patient interest in, concern about, and individual risk of drug toxicity. The decision about when to start therapy is a balancing act between factors favoring deferring therapy, such as a better quality of life and less risk of developing resistance, and the main factor favoring initiation of therapy, which is avoidance of deterioration of the immune system to the point that it cannot be rescued with antiretroviral therapy. There are data that support earlier initiation of therapy than the recommendations above advise, such as the Wang study, which showed a higher mortality for people who were started on HAART later, and other evidence that will be factored into future recommendations. There will no doubt be modifications from time to time in the recommendations based on studies of measures of viral replication and immunological function, the availability of clinically useful resistence studies, and with increased convenience and lower toxicity of available therapies. Similarly, the recommendations for initial therapy for HIV have evolved over time, with the current regimens being a choice of a ritonavir-boosted protease inhibitor plus two NRTIs, or a nonnucleoside reverse transcriptase inhibitor plus two NRTIs. Previously recommended regimens, such as 4-drug regimens, 3-NRTI regimens, and single-drug regimens, are no longer considered optimal. - Nunh-huh 04:01, 14 Jun 2005 (UTC)
- Further to this, here's the current AIDS treatment guidelines from the US Department of Health and Human Services. From page 8:
- When should therapy be started in patients with established asymptomatic infection?
- The Panel reaffirms the desirability of initiating therapy before the CD4 cell count falls below 200 cells/mm3. In addition, there are inconsistent data documenting added value in treating before the count falls below 350 cell/mm3, but some clinicians opt to consider treatment in patients with CD4 count >350 cell/mm3 and HIV-RNA >100,000 copies/mL. A review of the literature on this issue can been seen in the When to Treat: Indications for Antiretroviral Therapy section.
- Like I said, the jury's still out on this. -- Robert Merkel 03:53, 14 Jun 2005 (UTC)
- Going back to the original point, there's not much directly on this in the guidelines but they do say the following, in regards to reasons for commencing therapy: "Potential Risks of Deferred Therapy include:...the increased risk for HIV transmission to others during a longer untreated period.". So these guys seem to think that antivirals can reduce the risk of HIV transmission, and that's a relevant factor for considering when to commence treatment. -- Robert Merkel 04:04, 14 Jun 2005 (UTC)
Alternative theories
The purpose of this section appears to be to ridicule some Nobel laureates and the Murdoch press, without actually stating their views. Words like, mainstream, activists, dissidents, and AIDS denialism are all emotive words, which judge positions that are not presented. I am deleting it Joe Merkel 02:34, 12 Jun 2005 (UTC)
Main article: AIDS reappraisal
A few scientists and AIDS activists continue to question the connection between HIV and AIDS, the very existence of HIV, or of an independent AIDS disease. The validity of current testing methods is also questioned. Dissident scientists report that they are usually not invited to attend AIDS conferences and are not granted research funding from most mainstream sources. Prominent members of this group are virus researcher Peter Duesberg and Nobel Prize laureate Kary Mullis. These theories have been in the field for at least 15 years, and have found little support beyond the original circle of advocates. They gained prominence when they were promoted, for reasons which have never been made clear, by sections of the Murdoch press, such as the Sunday Times and The Australian.
Dr. Robert E. Willner caught the attention of the Spanish media, when in 1994 he inoculated himself with the blood of Pedro Tocino, an HIV positive hemophiliac on live TV. Dr. Willner died of a [[heart attack]] in 1995.
Mainstream AIDS activists characterize the position of these dissidents as " AIDS denialism," and believe their public proselytization for their various theories is destructive to the adoption of appropriate preventive and therapeutic measures. Active advocacy of these theories is largely confined to radical gay activist groups such as ACT-UP in San Francisco. (Not to be confused with ACT-UP/Golden Gate, which split from ACT-UP San Francisco in 1990, and changed its name in 2000 to avoid association with ACT-UP/San Francisco's non-mainstream views). As with the enthusiasm for alternative therapies, advocacy of unorthodox views about AIDS has declined with the increasing success of orthodox medical approaches to AIDS therapies.
Origins edit
This is the AIDS article, so the first point is that "AIDS spread initially in West Africa." As this is the habitat of the common chimpanzee genetic comparisons of HIV and SIV were done by the team at University of Alabama. 1999 is the date of publication not when the research was done. The researchers have wisely avoid speculation about how the transfer from chimpanzee to human occured. Weiss, a leading expert in AIDS, suggests the butchering of chimpazees for meat is a possiblity. Beliefs about prostitutes are unsupported by evidence. The polio vaccine theory has also been investigated and discarded. An encyclopedia is not a repository of every discredited belief, blind alley or red herring. Stick to the facts than can be referenced.
The is no reason to repeat the artists impression of HIV. It is already on the HIV article. Joe Merkel 16:56, 12 Jun 2005 (UTC)
What is a section about the origins of HIV doing in the AIDS article? Is the correct place the HIV article. Sci guy 14:12, 13 Jun 2005 (UTC)
Treatments and vaccines edit
I have divided this into two sections, because treatments are for people with AIDS and vaccines are intended to prevent HIV - actually vacines probably belong in the HIV article.
I have edited to the 2002 treatment guidelines and linked to the Antiretroviral drug article. Statements like "The majority of the world's infected individuals, unfortunately, do not have access to medications and treatments for HIV and AIDS." are demeaning, racist, and inaccurate. The fact is the majority of the HIV infected people in the world do not meet the current treatment guidelines! Joe Merkel 17:05, 12 Jun 2005 (UTC)
Treatments and Vaccines.
Section excised until dispute solved. Please write alternate versions here, discuss and come to agreement. HINT: fact checking is good.-- Tznkai 16:17, 15 Jun 2005 (UTC)
Antiretroviral regimens are complex, have serious side effects, pose difficulty with adherence, and carry serious potential consequences from the development of viral resistance because of nonadherence to the drug regimen or suboptimal levels of antiretroviral agents. Patient education and involvement in therapeutic decisions are critical. Treatment should usually be offered to all patients with symptoms ascribed to HIV infection. Recommendations for offering antiretroviral therapy among asymptomatic patients require analysis of real and potential risks and benefits. Panel on Clinical Practices for Treatment of HIV. September 2002
There is ongoing research into developing a
vaccine for HIV and in developing new anti-retroviral drugs. Human trials are currently underway. Research to improve current treatments includes simplifying current drug regimens to improve adherence and in decreasing side effects.
VIRxSYS Corporation has developed an innovative HIV lentiviral vector, called VRX496, that can be used to combat the HIV virus. The method has entered Phase I clinical trials, and it is the first-ever use of a lentiviral vector in humans. If results are positive, the method might be proven an effective cure for the AIDS disease.
Ever since AIDS entered the public consciousness, various forms of alternative medicine have been used to treat its symptoms. In the first decade of the epidemic when no useful conventional treatment was available, a large number of PWAs experimented with alternative therapies of various kinds, including massage, herbal and flower remedies and acupuncture, to either combat the virus or to relieve related symptoms. None of these were shown to have any genuine or long-term effect on the virus in controlled trials, but they may have had other quality of life-enhancing effects on individual users. Interest in these therapies has declined over the past decade as conventional treatments have improved. They are still used by some people with AIDS who do not believe that HIV causes AIDS. Alternative therapies such as massage, acupuncture and herbal medicine are still used by many sufferers in conjunction with other treatments, mainly to treat symptoms such as pain and loss of appetite. People with AIDS, like people with other illnesses such as cancer, also sometimes use marijuana to treat pain, combat nausea and stimulate appetite.
Alternate version: Newer treatments, however, have played a part in delaying the onset of AIDS, on reducing the symptoms, and extending patients' life spans. Over the past decade the success of these anti-retroviral treatments in prolonging, and improving, the quality of life for people with AIDS has improved dramatically.
Current optimal treatment options consist of combinations ("cocktails") of two or more types of anti-retroviral agents such as two nucleoside analogue reverse transcriptase inhibitors (NRTIs), and a protease inhibitor or a non nucleoside reverse transcriptase inhibitor (NNRTI). Patients on such treatments have been known to repeatedly test "undetectable" (that is, negative) for HIV, but discontinuing therapy has thus far caused all such patients' viral loads to promptly increase. There is also concern with such regimens that drug resistance will eventually develop. In recent years the term HAART (highly-active anti-retroviral therapy) has been commonly used to describe this form of treatment. The majority of the world's infected individuals, unfortunately, do not have access to medications and treatments for HIV and AIDS.
There is ongoing research into developing a vaccine for HIV and in developing new anti-retroviral drugs. Human trials are currently underway. Research to improve current treatments includes simplifying current drug regimens to improve adherence and in decreasing side effects.
VIRxSYS Corporation has developed an innovative HIV lentiviral vector, called VRX496, that can be used to combat the HIV virus. The method has entered Phase I clinical trials, and it is the first-ever use of a lentiviral vector in humans. If results are positive, the method might be proven an effective cure for the AIDS disease.
Ever since AIDS entered the public consciousness, various forms of alternative medicine have been used to treat its symptoms. In the first decade of the epidemic when no useful conventional treatment was available, a large number of PWAs experimented with alternative therapies of various kinds, including massage, herbal and flower remedies and acupuncture, to either combat the virus or to relieve related symptoms. None of these were shown to have any genuine or long-term effect on the virus in controlled trials, but they may have had other quality of life-enhancing effects on individual users. Interest in these therapies has declined over the past decade as conventional treatments have improved. They are still used by some people with AIDS who do not believe that HIV causes AIDS. Alternative therapies such as massage, acupuncture and herbal medicine are still used by many sufferers in conjunction with other treatments, mainly to treat symptoms such as pain and loss of appetite. People with AIDS, like people with other illnesses such as cancer, also sometimes use marijuana to treat pain, combat nausea and stimulate appetite.
Responses:
- I don't think anything is to be gained by discussing with radical AIDS denialists like Sci Guy and Fred2005. Time and again we have patiently explained things to them and provided sources, yet they still delete any information about benefits of AIDS treatment while adding their bullshit claims such as "AIDS is completely confined to gays and drug users in the US". I'm curious why you cut and pasted the AIDS denialist version of the section here, as opposed to the scientific consensus version. You don't get it, this isn't a legitimate dispute. It's the overwhelming scientific consensus versus a few fringe activists. Rhobite 16:36, Jun 15, 2005 (UTC)
- You're right. I don't get it because I'm not a scietist myself, and I don't magically know what the consensus is. I'm not here to cry what is true, but I do know when something needs discussion and when something doesn't. Alternate version is now up.-- Tznkai 16:55, 15 Jun 2005 (UTC)
September 2003 treatment guideline from Body
This link was in the references. Is it one of the AIDS denialist websites? They seem to be pushing the same line about defering treatment. [1]
- Doctors still disagree about when is the best time to begin HIV treatment, also called anti-retroviral therapy. You and your doctor will need to determine this together, but there are some respected guidelines. Be aware that these guidelines are regularly updated and are just suggestions based on the most recent research, and are not hard and fast rules.
- For example, the U.S. government's Department of Health and Human Services recommends that you begin HIV treatment if you have any serious symptoms, or if your T-cell count falls below 200. When your T-cell count drops below 200, you risk possibly irreversible health problems both before and after you begin treatment
Current Guidelines Recommend
- If your T-cell count is 350 or above, do not start medications unless your viral load is 55,000 or higher.
- If your T-cell count is between 200-349, treatment should be considered.
- If your T-cell count is below 200, treatment is indicated.
If the U.S. government's Department of Health and Human Services says do not do not start medications, if your T-cell count is 350 or above unless your viral load is 55,000 or higher - then who is advocating early treatment?
As editors it is our role to source the facts. Joe Merkel 15:08, 16 Jun 2005 (UTC)
- Considering treatment when CD4 count is between 200-350 is the current consensus in the various guidelines. Unfortunately, denialists like you look at any change in medical consensus as conclusive proof that doctors don't know what they're talking about. I have one more bone to pick with your edits: You added the text "Many people believe that newer treatments have played a part in delaying the onset of AIDS, on reducing the symptoms, and extending patients' life spans, although experts describe the data as inconclusive". I see that the word "inconclusive" came from the treatment pocket guidelines. The guidelines merely say that the data is inconclusive about whether to start treatment when CD4+ is above 350. You, however, made a misrepresentation (hopefully not deliberate) and claimed that the pocket reference guide was stating that the overall efficacy of HAART was "inconclusive". Hopefully this misrepresentation will stop, as I've linked to two large studies which show that HAART is effective, and which carry much more weight than a pocket treatment card. Rhobite 16:20, Jun 16, 2005 (UTC)
Aids and homosexuality
I think its important to talk about this, because atleast in the united states, there is a link in peoples minds, and there is a statistical link that it happens fairly often. Any takers?-- Tznkai 19:32, 13 Jun 2005 (UTC)
- There's no MEDICAL link, so I don't see your point, unless statistics is enough for you, in that case there's also a statistical link between the number of people with IQs below 100 and the number of conservative christians in this country,
- coincidence??
-any takers?-- 172.152.58.17 19:38, 13 Jun 2005 (UTC)
- Its important because this isn't a medical textbook, its an encylcopedia, and not putting the information in here leaves people trying to decide if Fred Phelps knows what he's talking about without a resource that leads them quickly to evidence to the contrary.-- Tznkai 19:49, 13 Jun 2005 (UTC)
- As I stated above, I think a summary of all the statistics put in laymens terms in it's own section of this document that publishes all the relevant data without singling out a particular minority for special notice would be the most balanced and neutral way of presenting this information and would still allow people to decide if Fred Phelps knows what he is talking about, without actually pandering to anyone's prejudices.
Axon 14:16, 14 Jun 2005 (UTC)
- Sounds good to me. Where would it go?-- Tznkai 16:58, 15 Jun 2005 (UTC)
- As I stated above, I think a summary of all the statistics put in laymens terms in it's own section of this document that publishes all the relevant data without singling out a particular minority for special notice would be the most balanced and neutral way of presenting this information and would still allow people to decide if Fred Phelps knows what he is talking about, without actually pandering to anyone's prejudices.
Axon 14:16, 14 Jun 2005 (UTC)
In the United States, 75% or reported AIDS cases were attributed to male-to-male sexual contact or injection drug use. These are the two original risk groups identified in 1983, before HIV blood screening was available. This is very different from Africa. I consider "male-to-male sexual contact or injection drug use" to be a NPOV description of behaviour Sci guy 03:01, 14 Jun 2005 (UTC)
- Sci-guy, that statistic is completly out of context. Reading through the talk history I can see that it came out of a legitimate attempt to neutralize an inserted statistic, but it equivocates malemale and drug users!-- Tznkai 13:54, 14 Jun 2005 (UTC)
Fred2005's nonsense
This article is getting torn up by Fred's edits. He is replacing well-written paragraphs with dire warnings about the dangers of HIV treatment and claims of controversy about early treatment. Of course we should mention the most current guidelines for starting treatment, but in a neutral manner (and without removing information on the benefits of HAART). Rhobite 16:33, Jun 14, 2005 (UTC)
- I believe Fred2005 has broken the 3RR rule [2] [3] [4] [5] with his last edit. Axon 16:39, 14 Jun 2005 (UTC)
Removal of talk page comments
Uh, where did my remarks on this talk page go? It seems they have been completely deleted by SciGuy [6]. They are not in the talk archives or the NPOV dispute branch SciGuy created. Axon 16:42, 15 Jun 2005 (UTC)
What has happened here??
A couple of weeks ago this article was great. It was comprehensive, well written, flowed well... Now it's a mess. The writing is terrible, relevant information has been cut, the flow is off... What's going on? Exploding Boy 17:10, Jun 15, 2005 (UTC)
- It has been invaded by the POV warriors. The stench of POV is terrible. I think it is time for an RFM on some editors who remove valid information to suit their views.
JFW |
T@lk 18:04, 15 Jun 2005 (UTC)
- What he said. →Raul654 18:06, Jun 15, 2005 (UTC)
- I think it would be a good idea if someone creates a sub-page here with an older, un-POV'd version of this article and calls for a RfC. Axon 18:07, 15 Jun 2005 (UTC)
- I'm vaugley new. You mean this article was ok once upon a time? From where I started, I lost track of what the facts were since no one does any fact checking around here -- Tznkai 18:12, 15 Jun 2005 (UTC)
- According to ExplodingBoy it was: any comments ExplodingBoy? Axon 18:16, 15 Jun 2005 (UTC)
- Mediation.. I wish I was as patient as you guys. I don't think this will stop until editors like Sci Guy and Fred2005 are banned from editing AIDS-related articles. Rhobite 18:14, Jun 15, 2005 (UTC)
I've reverted to EB's version from May 18 (with a few tweaks to incorperate the new pictures and remove the depricated lists). →Raul654 19:01, Jun 15, 2005 (UTC)
- Fabulous. I was stunned at first over the massive rollback, and reasserted the NPOV flag, but once I read it, I reverted my flag. It's pretty darn good. Whig 19:45, 15 Jun 2005 (UTC)
- Unfortunately some of Sci Guy's stuff is left in the article, e.g. the "AIDS is defined as occuring" gibberish, direct out of context quotes from random NIH reports (passed off as Sci Guy's own words), Bangui definition, etc. Still needs some work but overall this version is better than the one from the past few days. Rhobite 20:39, Jun 15, 2005 (UTC)
- The Bangui definition and discrepancy with HIV antibodies should not be in the intro. A number of tropical illnesses or combinations thereof could easily fulfil the Bangui criteria, fuelling Sci Guy's nonsense about discrepancy between clinical and laboratory AIDS.
- It should be mentioned that Koch's postulates have been met hundreds of times over for AIDS, confirming HIV as an agent and effectively relegating the Duesberg psychos to the history of medicine. JFW | T@lk 20:46, 15 Jun 2005 (UTC)
- I agree that the Bangui def is out of place in the intro, but it is definitely significant for a history section or "History of AIDS" article IMHO.
- As for the Koch's postulates argument... well, yes, that's also worth a mention, but I just know there's a POV battle looming if we use it to clobber alternate hypotheses. - jredmond 21:03, 15 Jun 2005 (UTC)
- Of course the Bangui def should be here, just in the history section. As for Koch's postulates, we should mention which study first fulfilled them; this the bread & butter of clinical microbiology. JFW | T@lk 22:34, 15 Jun 2005 (UTC)
- Any chance that that study (or at least an abstract thereof) would be online? As long as we even imply that there's a connection between HIV and AIDS, we'll have POV warriors coming through, but a link to a peer-reviewed study should dramatically reduce their number and severity. - jredmond 22:57, 15 Jun 2005 (UTC)
- PMID 8902385 mentions it, but I can't find the studies it refers to. I'll go through the article and come back to this page. Here is something more interesting. JFW | T@lk 23:48, 15 Jun 2005 (UTC)
- I do like the second one better... but hell, let's link 'em both. - jredmond 23:58, 15 Jun 2005 (UTC)
- Sounds like a good idea--but be forewarned: peer-reviewd studies don't seem to do much good in convincing idealogues of scientific evidence. Carl Henderson 23:46, 15 Jun 2005 (UTC)
- I know. But it's pretty tough to mess with links to peer-reviewed studies without raising a lot of vandal/POV warrior flags and attracting a whole lot of negative attention. - jredmond 23:58, 15 Jun 2005 (UTC)
- Thanks for remembering the images. I went back in and adjusted the image sizes. The "HIV Daughter Particles" image was sized at higher than its native resolution. I also upsized the "HIV Viron" image so that all the the text could be read (at least on my screen). Carl Henderson 23:46, 15 Jun 2005 (UTC)
Oh yeah. That's more like it. Exploding Boy 00:55, Jun 16, 2005 (UTC)
I think this statement needs to be reworded for NPOV: "The situation in South Africa, where President Thabo Mbeki shares the beliefs of "AIDS denialists," is a negative influence and neglection of the fact that 4.7 million infections took place for 2002." Whig 03:04, 16 Jun 2005 (UTC)
Japan's tainted blood scandal
Please see [7]. Exploding Boy 02:24, Jun 16, 2005 (UTC)
- One of the most famous hemophilia patients was Stephen Christmas, namesake of Christmas disease. He is a case in point. JFW | T@lk 15:42, 16 Jun 2005 (UTC)
- Yes... but he's not Japanese and he wasn't a part of the Japanese tainted blood scandal... I"m really looking for imput on how to title the article or where to find it if one already exists. Exploding Boy 18:44, Jun 20, 2005 (UTC)
Please see HIV-tainted blood scandal (Japan). Exploding Boy 00:51, Jun 21, 2005 (UTC)
undetectable
I have a problem with:
"Patients on such treatments have been known to repeatedly test "undetectable" (that is, negative) for HIV, but discontinuing therapy has thus far caused all such patients' viral loads to promptly increase"
Does "have been known" mean that this is an unusual or rare outcome?
I assume the intention is to claim that viral load blood test is undetectable rather suggesting that such treatments mean a person is negative for HIV on the antibody test.
I suggest we need a source reference so we can edit this to avoid misunderstanding Joe Merkel 15:33, 16 Jun 2005 (UTC)
- No, antibodies persist. Viral load has a lower limit of detection, and the virus may be reactivated if HAART is stopped. There is nothing counterintuitive about this, and may not even need sourcing. Antiretrovirals suppress viral replication, sometimes to the point that the viral load is under the detection limit, but when discontinued the virus comes back. Sure. JFW | T@lk 15:40, 16 Jun 2005 (UTC)
Joe, I am sick of people coming in to the treatment section and "nerfing" it with vague phrases like "Many people believe that newer treatments have played a part in delaying the onset of AIDS". Peer-reviewed research and clinical trials should not be described as "many people". Many times over, studies have showed that patients who properly adhere to therapy have much lower viral loads, higher CD4 counts, and longer survival times. I am linking to two of these studies so please cut out the vague rewrites. [8] [9]
Also, please stop mentioning the dangers of antiretroviral therapy before it is even described. HAART is not perfect. I'm not trying to hide mention of these problems, but mentioning them before HAART is even described is confusing and dismissive. Rhobite 16:01, Jun 16, 2005 (UTC)
- Rhobite, could you cite PMID abstracts scientifically in a section called "References" and using footnotes? This massively improves the credibility of your edits. See obesity for an example. JFW | T@lk 16:22, 16 Jun 2005 (UTC)
- The automatic footnoting system is currently a huge pain to work with, due to the lack of automatic renumbering. With the article under attack by people who don't mind removing references, I think using the system would be futile. I will add them as general references with no footnotes, however. Rhobite 16:44, Jun 16, 2005 (UTC)
- Rhobite, new users don't know how to properly refrence. You do. Show a better example.-- Tznkai 16:49, 16 Jun 2005 (UTC)
- I just added a references section. If that isn't good enough for you, feel free to implement automatic footnoting. As you've only been around here for a couple weeks you may not yet realize that automatic footnotes are close to impossible to maintain in a rapidly changing article such as this one. As I said, I'm not being lazy, I think using automatic footnotes would be futile right now.
- I prefer to spend my time on this article refuting fringe opinions about AIDS, as opposed to constantly reordering footnotes. How you choose to spend your time is your business. I'd appreciate fewer patronizing remarks, and more beneficial contributions out of you. Rhobite 17:03, Jun 16, 2005 (UTC)
- Good call on the named references, I will add those to the treatment section. Rhobite 18:39, Jun 16, 2005 (UTC)
Liver Failure
Under paragraph two of "AIDS epidemic," the article currently states, "In the United States, the most common cause of death for people with AIDS is liver failure caused by antiretroviral drugs." I'm very skeptical of this statement--especially considering many people with AIDS in the US are also co-infected with Hepatitis B or C.
The only source I can find for the liver failure mortality claim is a University of Pittsburgh Medical Center press release [10] highlighting a study by Dr. Amy Justice, presented at 14th International AIDS Conference in Barcelona (2002). She is quoted, saying, "[f]urthermore, the fact that the most common current cause of death among people with HIV is liver failure suggests that liver injury may be a major limiting factor in the effectiveness of current HIV treatment." That quote was then picked up in several news articles and ended up on lots of the "HIV doesn't cause AIDS" websites.
Can anyone verify that liver failure caused by antiretroviral drugs is the most common cause of death for people with AIDS in the US? I tried, and I can't. Carl Henderson 00:14, 17 Jun 2005 (UTC)
- In any case, even if antiretrovirals do ultimately end up killing people through liver failure, it doesn't necessarily follow that antiretroviral treatment is bad; AIDS may well have killed them sooner and more painfully...-- Robert Merkel 03:08, 17 Jun 2005 (UTC)
- Shouldn't matter, we just need the facts, right?-- Tznkai 03:19, 17 Jun 2005 (UTC)
- As long as they're presented accurately and neutrally. Some people have a tendency to put the cart before the horse when describing the negative aspects of antiretroviral drugs. Rhobite 03:33, Jun 17, 2005 (UTC)
- My point is I don't think "most common current cause of death among people with HIV is liver failure" is "the facts." I've only found one primary reference to it--and that was a press release--not the original study cited. I'm looking for some more sources one way or another.
- Nevertheless, the way the article currently phrases the "liver failure" claim is wrong. With the widespread co-infection of Hepatitis B or C among many groups of AIDS patients in the US, it would be impossible to ascribe all deaths from liver failure to antiretrovirals. Carl Henderson 15:14, 17 Jun 2005 (UTC)
- Whether retrovirals are "good" or "bad" isn't a judgment that Wikipedia can make. We can and should cite references showing their effects on mortality rates from AIDS as well as from direct toxicity. I think that any reasonable person would hope that less toxic effective treatments would eventually be found, we ought not to sanitize the effects (positive or negative) from AZT and HAART, etc. Whig 03:49, 17 Jun 2005 (UTC)
It's certainly not true that "liver failure caused by antiretroviral drugs" is the leading cause of death in HIV infected people in the U.S. And we have no citation for that assertion. I suspect what's happened is someone has taken a study in which the most common cause of non-AIDS-related death in AIDS patients is liver failure, added their erroneous assumption that this was due to drugs rather than co-infection with hepatitis B or C, and asserted it here as fact. One study showing results capable of such misinterpretation (but in France rather than the U.S.) is here, and another one among women here. In all such studies, liver failure remains one of the more common types of non-AIDS-related deaths, but non-AIDS-related deaths are dwarfed by AIDS-related causes. A possible explanation of the high incidence of renal and hepatic failure is suggested here to be a rising proportion of drug addict in the population. But we shouldn't be misinterpreting all liver failure in the HIV infected as drug-induced. - Nunh-huh 21:41, 17 Jun 2005 (UTC)
- I've been doing some research and have now found studies both confirming and disconfirming the "In the United States, the most common cause of death for people with AIDS is liver failure" part of the statement, but not the "caused by antiretroviral drugs" clause. Note that I've included references to two studies looking at the Mortality 2000 study group in France. I'm assuming that the demographics of AIDS patients in France are not that different from those in the US.
- First the disconfirming studies:
- Changes in Mortality Related to Human Immunodeficiency Virus Infection: Comparative Analysis of Inpatient Deaths in 1995 and in 1999–2000
- Clinical Infectious Diseases, 2003;36:1030-1038
- Mamta K. Jain, Daniel J. Skiest, Jeff W. Cloud, Charu L. Jain, Dennis Burns, and Ruth E. Berggren
- ABSTRACT: We conducted a retrospective chart review of human immunodeficiency virus (HIV)–infected patients who died in 1995 and in 1999–2000. We found an increase in the proportion of patients who died from an illness that was not related to acquired immunodeficiency syndrome (AIDS). Although there was a decrease in the prevalence of AIDS-defining illnesses, >85% of patients died with CD4 counts of <200 cells/μL. The leading cause of death was Pneumocystis carinii pneumonia (PCP). Nonadherence to therapy and new diagnosis of HIV infection were the leading reasons why patients were not receiving antiretroviral therapy. The leading causes of non–AIDS-related deaths in 1999–2000 were non–AIDS-defining infections and end-stage liver disease. At our hospital, PCP remains an important cause of death in the highly active antiretroviral therapy (HAART) era, possibly because >50% of HIV-infected patients who died were not receiving HAART. AIDS-defining illnesses continue to be a major cause of mortality in the HAART era in populations where access to care and adherence to HAART is limited.
- Causes of death among human immunodeficiency virus (HIV)-infected adults in the era of potent antiretroviral therapy: emerging role of hepatitis and cancers, persistent role of AIDS
- International Journal of Epidemiology, 2005 Feb;34(1):130-1.
- Lewden C, Salmon D, Morlat P, Bevilacqua S, Jougla E, Bonnet F, Heripret L, Costagliola D, May T, Chene G; Mortality 2000 study group
- ABSTRACT: Background-In the era of highly active antiretroviral therapy (HAART) mortality has decreased substantially among human immunodeficiency virus (HIV)-infected people with access to HAART, but there are concerns regarding co-morbidities and adverse effects of HAART, which may impair vital prognosis. The Mortality 2000 study examined the causes of death in HIV-infected adults at a national level in France in the year 2000. Methods-All French hospital wards known to be involved in the management of HIV infection were asked to notify prospectively the deaths that occurred in 2000 among HIV-infected adults. The causes of death were documented using a standardized questionnaire. Results-The 185 participating wards notified 964 deaths. The main underlying causes of death were AIDS-related (47%, non-Hodgkin's lymphoma: 23%), viral hepatitis (11%, hepatitis C: 9%, hepatitis B: 2%), cancer not related to AIDS or hepatitis (11%), cardiovascular disease (7%), bacterial infections (6%), suicide (4%), and adverse effect of antiretroviral treatments (1%). Among AIDS-related deaths, HIV infection had been diagnosed recently in 20%. Smoking was recorded in 72% of cancer-related deaths and alcohol consumption in 54% of hepatitis-related deaths. Among non-HIV related deaths between 25 and 64 years, the proportion of infectious diseases (including HCV and HBV-related deaths) was higher in HIV-infected adults than in the general population. Conclusions-Improved strategies for detecting HIV infection before AIDS-defining complications occur are needed in the era of HAART. The prevention of non-AIDS related cancers, especially lung cancer, the management of non-Hodgkin's lymphoma, and of viral hepatitis are also important priorities.
- Causes and characteristics of death among HIV-1 infected patients with immunovirologic response to antiretroviral treatment
- Presse Medicale,. 2004 Dec 4;33(21):1487-92.
- May T, Lewden C Bonnet F, Heripret L, Bevilacqua S, Jougla E, Costagliola D, Morlat P, Salmon D, Chene G; Groupe d'Etude Mortalite 2000
- ABSTRACT: To analyse the causes of death among HIV-infected adults in France in the year 2000. METHODS: Based on data from a national survey, our study describes and analyses the causes and characteristics of patients with immunological and virological response (CD4>200/mm3, ARN-HIV<500 copies/mL), who died during antiretroviral treatment. RESULTS: Among a total of 964 deaths registered, data on 864 cases were available for analysis. One hundred forty-nine patients (17%)were immunovirological responders. The underlying causes of death were non AIDS-defining malignancies for 36 (24%), mainly due to lung cancer (16 cases), hepatocarcinoma (7) and ano-rectal carcinoma (3), AIDS for 22 (15%), mainly due to Non Hodgkin Lymphoma (10 cases) and uterine cancer (3), cardiovascular diseases for 22 (15%), post hepatitis C hepatic failure for 16 (11%), suicide for 16 (11%), and bacterial infections for 14(9%). When comparing characteristics of death in the 149 responders versus the 715 other patients, the responders were significantly more frequently: co-infected by HCV+ (45 vs. 33%), injected drug addicts (40 vs. 27%),alcoholics (38 vs. 28 %), and dyslipidemics (19 vs. 11%). In 2000,around 20% of registered deaths of HIV patients in France had occurred among good immunovirological responders. CONCLUSION: To further reduce mortality among such efficiently treated patients, attention must be focused on treatable conditions such as hepatitis C, dyslipidemia and on the prevention of malignancies such as lung cancer and cervical or ano-rectal carcinoma.
- (abstract only--article in French)
- Now for a confirming study:
- Increasing Mortality Due to End-Stage Liver Disease in Patients with Human Immunodeficiency Virus Infection
- Clinical Infectious Diseases, 2001;32:492-497
- Ioana Bica, Barbara McGovern, Rakesh Dhar, David Stone, Katherine McGowan, Rochelle Scheib, and David R. Snydman
- ABSTRACT: Highly active antiretroviral therapy has decreased human immunodeficiency virus (HIV)–associated mortality; other comorbidities, such as chronic liver disease, are assuming greater importance. We retrospectively examined the causes of death of HIV-seropositive patients at our institution in 1991, 1996, and 1998–1999. In 1998–1999, 11 (50%) of 22 deaths were due to end-stage liver disease, compared with 3 (11.5%) of 26 in 1991 and 5 (13.9%) of 36 in 1996 (P = .003). In 1998–1999, 55% of patients had nondetectable plasma HIV RNA levels and/or CD4 cell counts of >200 cells/mm3 within the year before death. Most of the patients that were tested had detectable antibodies to hepatitis C virus (75% of patients who died in 1991, 57.7% who died in 1996, and 93.8% who died in 1998–1999; P = NS). In 1998–1999, 7 patients (31.8%) discontinued antiretroviral therapy because of hepatotoxicity, compared with 0 in 1991 and 2 (5.6%) in 1996. End-stage liver disease is now the leading cause of death in our hospitalized HIV-seropositive population.
- Plus a link to a Powerpoint presentation citing several studies (that I've not had a chance to run down) also supporting the "liver failure" claim:
- Liver disease has emerged as a major cause of mortality in the HAART era.
- http://www.roche-hiv.com/roche-in-hiv/Conferences/Documents/02-Dieterich-Show.ppt
- My conclusion--I don't think the research firmly supports the "liver failure" claim, but I also don't think I'm qualified to make any such conclusion as far as Wikipedia is concerned.
- Help. Carl Henderson 05:40, 18 Jun 2005 (UTC)
"AIDS results from..."
This may have been discussed before, but does anyone think the sentence at the top
"AIDS results from an infection of HIV, the Human Immunodeficiency Virus, although some debate this."
is really poor? I mean, the first part says - "HIV results in AIDS" and the second - "It's debatable that HIV results in AIDS". Can't we say something like "AIDS results from an infection of HIV, the Human Immunodeficiency Virus. Though the later has been widely credited, some still debate the origin of AIDS." Or maybe even take out "although some debate this." all together from the beginning and add it as a counter-point later in the article. Having it in the intro just makes a weak impression for the everything else. JoeSmack (talk) 15:32, Jun 17, 2005 (UTC)
I have never had a problem with "HIV causes AIDS". It is the same as "smoking causes lung cancer" or "speeding causes road accidents". The October 2004 version from U.S. Department of Health and Human Services is as follows:
- A positive HIV test result means that you are infected with HIV (Human Immunodeficiency Virus), the virus that causes AIDS (Acquired Immune Deficiency Syndrome). Being infected with HIV does not mean that you have AIDS right now. However, if left untreated, HIV infection damages a person’s immune system and can progress to AIDS. [11]
I was surprised by the "can" in "HIV infection damages a person’s immune system and can progress to AIDS". But the issue is not what you or believe, we are editors searching for facts that can be verified. So I agree with you that "although some debate this." is really poor. Who debates this? On what basis? When? As we are reminded each time we edit - "Please cite your sources so others can check your work." Sci guy 16:31, 17 Jun 2005 (UTC)
- I'm not sure how much more factual you can get than U.S. Department of Health and Human Services.
JoeSmack
(talk) 16:36, Jun 17, 2005 (UTC)
- The UN? I think Sci guy was referring to the "debate on this" part.-- Tznkai 16:40, 17 Jun 2005 (UTC)
- and the reason that "can" is in there is because of long-term HIV nonprogressors - HIV does lead to AIDS for a vast vast majority of those infected when left untreated. JoeSmack (talk) 16:41, Jun 17, 2005 (UTC)
I have removed the offending phrase (which I wrote in the first place). →Raul654 17:18, Jun 17, 2005 (UTC)
Major changes
Alright guys, don't be scared, but I printed this thing out and started using a red pen. Mostly it has been removing things stated as facts that have no cite, things that don't belong in the article (the prevention section has a stupidly long thing on company condom testing), and things that should be moved. I am doing it in sections so that people can see the changes more easily.
I've gotten about halfway through the article with the red pen, and will finish and add the last half after i change the first half on here. Feel free to talk about the changes. JoeSmack (talk) 17:29, Jun 17, 2005 (UTC)
- i reverted one part where breastmilk etc. was deleted from the prevention section. it is really important info but it has no cite. please please someone find one and put it in so we can use it. JoeSmack (talk) 18:02, Jun 17, 2005 (UTC)
man, WTF guys? anyone notice that the Origin of AIDS section, probably one of the most important, has NO CITES whatsoever? you guys are telling me there is no book on the history of AIDS out there? -- someone please take this one on, i'm not even going to touch it cause i'd just delete the whole thing (important yes, but there are no cites). JoeSmack (talk) 18:12, Jun 17, 2005 (UTC)
- the Current medical understanding of AIDS section is just no cite after no cite. They just state them like they are facts or says 'studies have shown'. This is depressing guys, i'm not touching this thing either. JoeSmack (talk) 18:17, Jun 17, 2005 (UTC)
about that "devistating" remove. 23 million people in 24 years. imagine in 24 years from now you went to washington. everyone there would be dead. went to utah, everyone there would be dead. nevada. oregon. north dakota, nebraska.... doesn't that seem devistating? am i pushing the line with that word? JoeSmack (talk) 18:22, Jun 17, 2005 (UTC)
alright, I cant stand this ridiculas lack of citing sources. i'm stopping and continuing tomorrow or something. i'll be around if anyone wants to talk about the changes i've already made. JoeSmack (talk) 18:26, Jun 17, 2005 (UTC)
- Of course I agree with you, it is devastating. But it's POV for the article to use such words, even if most people would agree with them. The word doesn't enhance the sentence at all, it's just an appeal to emotion.
- About removing uncited parts. I agree that many parts of this article need citations. I don't know if the proper response is to simply remove them. Assuming that most of the contributions were made in good faith, I think it might be better to leave them in the article for the time being, and make a list of these claims which need to be cited. Then we can simply check things off the list once they are verified. Whether we leave them in the article or remove them, I think we need a list of uncited claims. People tend to forget about text once it's removed from an article, so we should keep track of these claims with the intention of replacing them. Would you be interested in helping to make this list?
Rhobite 18:34, Jun 17, 2005 (UTC)
- if you leave uncited parts until they are verified it can only cause problems. for instance, "AIDS has been correlated in men between 21 and 31 to higher speeding practices in cars." -- I made that up, it's bullshit. People who spread misinformation about AIDS do dumb stuff like this all the time, and to leave it there would be a disservice to people trying to educate themselves on AIDS everywhere. We shouldn't selectively decide 'which are probably true' and which aren't, so I think the best solution right now is to delete them.
Facts sourced
Alrighty guys, i added sources for the 1 in 200 rate of HIV infect for a needle prick and prevention for mothers birthing and breastfeeding for infants. Any takers for other sourceless facts? I've got list of removed 'facts' on my talk page that just need sources to go back in... JoeSmack (talk) 21:43, Jun 17, 2005 (UTC)
- I'm working on the "liver failure" claim. I'll also check the "[i]n Africa, the most common cause of death for people with AIDS is Tuberculosis" while I'm at it. I'll see if I can run down some of the others while I'm researching those, too. Carl Henderson 22:15, 17 Jun 2005 (UTC)
- I've done some research on the "liver failure" assertion, and posted it above under the Liver Failure section in the talk. Carl Henderson 05:42, 18 Jun 2005 (UTC)
- Here's another factoid sourced to add to the list. A previous version of the article stated that "Blood tranfusions remain a major source of new HIV infections worldwide. WHO estimated in 2000, between 15% and 20% of new HIV infections worldwide were the result of blood transfusions, where the donors were not screened or inadequately screened for HIV."
- Not quite accurate. According to a 2000 WHO press release Blood Safety... For Too Few, "between 5% and 10% of HIV infections worldwide are transmitted through the transfusion of infected blood and blood products. WHO/UNAIDS estimate that 5.6 million new HIV infections occur annually." This number is consistant with the WHO Global Database on Blood Safety's Summary Report for 1999-1998 which estimates that 43% of the blood supply in developing nations is not screened for HIV or other blood transmissible infections.
- Carl Henderson 00:52, 20 Jun 2005 (UTC)
- More cites found:
- "Chances of HIV transmission from infected male to female in a single act of genital sex are quite low: it is estimated that under normal conditions, only about 1 in 1000 acts results in infection." and "Transmission of virus from females to males is even less likely, but still possible."
- Acording to the CDC table SciGuy added Friday, these numbers are correct. I'd suggest a rewrite to say something like, "According to the CDC estimates (reference the table here), chances of HIV transmission from infected male to female in a single act of unprotected genital sex are quite low; it is estimated that under normal conditions, only about 10 in 10,000 acts results in infection. Transmission of virus from females to males is only about half as likely--though still possible. Note that these CDC estimates are averages, and actual odds of transmission of HIV via a single sexual act can be affected by other factors, such as the viral load of the infected partner or the presence of abrasions or sores on the genitals of either of the sexual partners." And if this section is rewritten, it should also be made clear that the CDC figures are based on AIDS in America, and that the methods of transmission elsewhere may not show the same pattern.
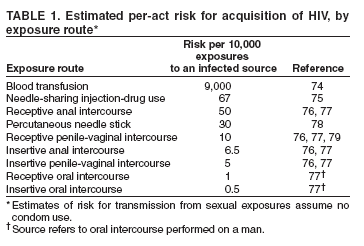{kind=link}
- One other thing. Factors such as drug use and the presence of other sexually transmitted diseases can also increase the likelyhood of transmission of HIV. Carl Henderson 18:24, 20 Jun 2005 (UTC)
- "One study concluded that 7.8% of recently infected men in San Francisco were probably infected through oral sex."
- Dillon B, Hecht FM, Swanson M et al., Primary HIV infections associated with oral transmission, 7th Conference on Retroviruses and Opportunistic Infections, San Francisco, January 30th-February 2nd, 2000 (abstract 473).
- That single 2000 study doesn't tell the whole story, though. The Public Health Agency of Canada has a good (and refenced) summary of various studies concerning oral HIV transmission, Oral Sex and the Risk of HIV Transmission. Research summarized in that May 2004 article demonstrated a wide range of risk estimates. Studies of different cohorts of homosexual males showed that from 3.9% to 16.2% were infected via receptive oral intercourse. Studies of different cohorts of hetrosexual couples showed that anywhere from 0% to 6.7% of heterosexual females were infected via receptive oral intercourse. Finally the PHAC article the overall literature, and found, "exposure to HIV through unprotected oral intercourse as an independent risk factor for HIV acquisition in only three (12.5%) of 24 epidemiological studies designed to examine risk of HIV from different sexual exposures."
- "A study of Spanish men who knowingly engaged in oral sex with HIV+ partners identified no cases of oral transmission."
- Evaluating the risk of HIV transmission through unprotected orogenital sex, Del Romero J, Marincovich B, Castilla J et al., AIDS 2002;16(9): 1296-97. Note that the study doesn't just concern Spanish men; the article covers a cohort of "135 seronegative individuals (110 women and 25 men), whose only risk exposure to HIV was unprotected orogenital sex with their infected partner."
- Carl Henderson 18:20, 20 Jun 2005 (UTC)
Why the heck has Bangui worked its way back in?
I thought I'd dealt with the Bangui definition way back in this edit. Why has this complete red herring, complete with unsourced claims about half the AIDS cases in Africa, snuck its way back into the article? -- Robert Merkel 08:45, 19 Jun 2005 (UTC)
I agree. The 'Bangui definition' is not part of the current definition, neither is hemophilia, Haitian, or male homosexual. The current definition based on HIV antibodies, T cells and AIDS defining illnesses would be better. Sci guy 14:12, 19 Jun 2005 (UTC)
- For those new to this article, Sci guy was the major proponent of the "Bangui definition" stuff in the first place. Please stop playing games. -- Robert Merkel 01:43, 20 Jun 2005 (UTC)
- Yes, he has changed tactics. Now he simply cuts and pastes selected bits of CDC literature into the article, in an effort to decrease readability I guess. Rhobite 02:01, Jun 20, 2005 (UTC)
Africans & genetics
I have heard that Africans are more likely to contract AIDS due to genetic factors and that a minority of those with Scandinavian genes are immune to it. Perhaps we should include something about this? 207.224.198.170 16:50, 19 Jun 2005 (UTC)
- You're thinking of the CCR5-Delta32 mutation, which provides some protection against HIV infection and is more common in those of European descent. see the CCR5 page in OMIM or do a Medline search on "CCR5-Delta32". - Nunh-huh 05:14, 20 Jun 2005 (UTC)
Drowning in statistics and terminology
I'm assuming that Sci guy's new tactic is simply to drown readers in overwhelming statistics and impenetrable language, such as the new CDC graphic and the large lists of people infected per region and deaths per region. I'm not saying this data shouldn't be in there, but there seems to be an intentional campaign to (a) make it take up as much space as possible and (b) copy complex language directly from medical studies.
For example, we just rewrote the lead section by hand over the past few days. I think the new lead is pretty good. Sci guy replaced the lead section with this text, copied directly from the CDC's MMWR, a publication which is intended for medical professionals:
- "The etiologic agent of acquired immunodeficiency syndrome AIDS is a retrovirus designated human immunodeficiency virus HIV. The CD4+ T-lymphocyte is the primary target for HIV infection because of the affinity of the virus for the CD4 surface marker. The CD4+ T-lymphocyte coordinates a number of important immunologic functions, and a loss of these functions results in progressive impairment of the immune response."
This text is basically unreadable to a layperson. I'm concerned that now that the legitimate contributors are making an effort to cite sources, Sci guy has shifted tactics towards trying to make the article as unreadable as possible. Sci guy please use your own words. Other people have taken the time to do research and write in language that is comfortable to read. If you are not willing or capable of doing the same, I'd ask that you please stop editing this article. All of your recent edits have been simple cut and paste jobs. Rhobite 16:57, Jun 19, 2005 (UTC)
- If you check the archive, you will find that Sci guy was previously criticized for NOT including the statement "The etiologic agent of acquired immunodeficiency syndrome AIDS is a retrovirus designated human immunodeficiency virus HIV." Now he is being criticized for including it! Is this article intended to contain, current referenced facts - or readable misinformation? For example the lead section now contains the popular misconception that "AIDS is a disease characterized by the destruction of the human immune system." In fact it is only part of the immune system the CD4 T cells that are affected, and this is thought to result in a loss of cell mediated immunity, and therefore vulnerablity to certain specifc diseases and some cancers. The current focus of AIDS is the heterosexaul epidemic in sub Saharan Africa. Fred2005 11:27, 20 Jun 2005 (UTC)
- Fred, you are quoting out of context. At the time, Rhobite was making the point that Sci Guy was selectively quoting the CDC (and back then, we were making the point that the article was unreadable through his and your efforts). Now, as Rhobite said, Sci Guy has switched gear to swamping the article in medical jargon. As to "destruction of the immune system", that's a good enough approximation for an article introduction. Now, stop wasting our time, please. -- Robert Merkel 12:34, 20 Jun 2005 (UTC)
| This page is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| This is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 | Archive 2 | Archive 3 | Archive 4 | Archive 5 | Archive 6 | → | Archive 10 |
DO NOT EDIT OR POST REPLIES TO THIS PAGE. THIS PAGE IS AN ARCHIVE.
This archive page covers approximately the dates between 20 May, 2005 and 20 June, 2005
Post replies to the main talk page, copying or summarizing the section you are replying to if necessary.
New Images
I've added two images from the National Institute of Health. The first--"HIV Viron.png"--replaces the old "Aids virus.jpg" image. The new image is clearer and provides a better description of the anatomy of the HIV viron. The second image--"HIV Daughter Particles.jpg"--illustrates the text about replication of HIV after and initial infection (under the "Current medical understanding of AIDS" section).
Please be nice to the new images while waging revert wars... Carl Henderson 04:26, 4 Jun 2005 (UTC)
fred's edit
I have removed. "During situations where treatments are available many people are able to delay death between ten to twenty years after the development of AIDS." becuase there is no factual basis for this claim. Show me the reference to a ten year survival for antiretrovirals . if you want to make this claim.
Also I have added. "In a process still imperfectly understood, HIV infects the CD4 cells (also called T4 or T-helper cells) of the immune system" This is the current 2005 "scientific consesus". Fauci of NIH from memory.
I have a problem with "AIDS typically develops about ten years following HIV infection." I think ten years is probably the 50% survival - so half develop AIDS within 10 tears and after 10 years half have not developed AIDS. Calling a mid point of a range "typical" seems misleading as in fact very few people wil actually develop AIDS in years 10
Also "proper administration" of antiretroviral medicatiom, seems unnecesarily contentious. Is there evidence of improper adminstration - is it itended to suggest that all or some doctors are imcompetent?
Fred2005 14:49, 11 Jun 2005 (UTC)
Symptoms
I have a problem with this:
- HIV is transmitted by bodily fluids, such as blood, semen, breast milk, and vaginal secretions. It causes disease by infecting CD4+ T cells, a type of leukocyte (white blood cell) that normally coordinates the immune response to infection and cancer. When a person's CD4+ T cell count decreases sufficiently he or she is prone to a range of diseases that a healthy person's body is normally able to fight. These diseases include cancers and opportunistic infections, which are usually the cause of death in persons with AIDS. HIV may also infect brain cells, causing some neurological disorders.
How is this relevant to Symptoms of AIDS?
The whole issue is that the first symptom of AIDS is usually an AIDS defining illness. Two thirds of reported AIDS in the United States is on the basis of low CD4 cell count - these cases are all asymptomatic
Also opportunistic infections was replaced by AIDS defining illness back in 1993. Can we move with the times and keep up to date with the scientific consenus please?
If you read the Pneumocystis jiroveci pneumonia article you will see that we have all moved on from the earlier suggestions about opportunistic infections. Fred2005 16:00, 11 Jun 2005 (UTC)
Prevention
Deleted "There is now some evidence that treatment of already-infected people with antiretroviral drugs may reduce the transmission of HIV infection to their sexual partners, independently of other safer-sex precautions [9] ( http://en.wikipedia.org/wiki/AIDS#endnote_BBCHAARTspread). This may imply that aggressively treating existing HIV cases, in addition to protecting the uninfected population through education and safer-sex programs, may be more effective at preventing the spread of HIV that either of these alone."
The scientific consesus is that people on retrovirals should use condoms, even if their viral load is undetectable Joe Merkel 02:23, 12 Jun 2005 (UTC)
- I'm uncertain on how well-supported the evidence is on this point, but in general I think you're seeing a contradiction where none needs to exist. Even if the risk of transmission is reduced by treatment, it doesn't mean that you still wouldn't advise the use of condoms to reduce the risk further. So unless the evidence for this reduced transmission is marginal in and of itself, I think the appropriate action would be to reinstate the sentence and note that this doesn't make it wise for HIV-positive people to have unprotected sex. -- Robert Merkel 07:43, 12 Jun 2005 (UTC) (no relation)
- I agree with you that we cannot determine from the linked newspaper article how well-supported the evidence is on this point. But the treatment guidelines have changed so much since 1997 that this research is largly irrelevant. The hit hard, hit early glory days are gone, because the scientific consenus has accepted the many studies showing unnacceptably high drug toxicity. Joe Merkel 15:38, 12 Jun 2005 (UTC)
- Hmmm. For one thing, the study began in 1997; given that it was published in 2004 I would suggest that the data would go to at least 2002. Seconldy, the latest source Sci Guy has dragged up suggests that treatment with low viral loads and high CD4+ counts is recommended against, but it says that for people with high viral loads that whether to offer treatment is controversial, particularly when the CD4+ counts are above 350/mm3. So , on the basis of that link (and it appears to be current and from a relevant, reputable source) the science isn't settled on exactly when to start treatment, and there seems to be some consideration for treatment purely to reduce viral loads. -- Robert Merkel 07:13, 13 Jun 2005 (UTC)
- That is correct, Robert. Treatment purely to reduce viral loads in people who have not been diagnosed with AIDS is now considered controversial in the United States. This is a big change in direction since the 1997 treatment guidelines. I am happy to read your Taiwanese research if you have a reference. The BBC article did not name an author. Sci guy 13:50, 13 Jun 2005 (UTC)
- I think you're reading more into the description of "controversial" than you should. I suspect "controversial" in this context means that the evidence that treatment is beneficial is unclear, and therefore some substantial group of clinicians think it's worthwhile and others don't. The jury is still out. Have a look at some of the criteria on which the decision to treat might be based, though; it includes likelihood of compliance with treatment. I suspect there might be more to it than drug toxicity; treatment, particularly imperfectly-applied treatment, might promote drug resistance and reduce treatment options later. -- Robert Merkel 23:53, 13 Jun 2005 (UTC)
- No Robert, this is the jury report. Controversial means the jury considered the evidence and does not recommend treatment. This is your scientific consenus in action. Facts change the minds of scientists, juries and politicians. Sci guy 03:26, 14 Jun 2005 (UTC)
- That's not what the text indicates. If there were a scientific consensus that treatment was not indicated, that guide wouldn't use the world "controversial". Looks like it might be time to dig up more information...-- Robert Merkel 03:43, 14 Jun 2005 (UTC)
- "Controversial" is a highly charged word. We should simply report facts. The optimum time to begin therapy remains an unresolved issue. It is recognized that therapy should begin before there is an irreversible deterioration of the immune system, and recommendations have varied: in 1987, treatment was delayed until patients had developed clinical AIDS; in 1996, the "hit-early-hit-hard" premise prevailed, and patients were treated when their CD4 count was <500/cmL. The current recommendations call for an intermediate approach: patients with CD4 counts < 200 should be treated, patients with CD4 counts > 350 who are asymptomatic should not be, and the decision on when to initiate treatment for patients with CD4 counts between 200 and 350 is based on rate of CD4+ cell count decline, HIV load (>100,000 copies is the number for concern), pregnancy, and patient interest in, concern about, and individual risk of drug toxicity. The decision about when to start therapy is a balancing act between factors favoring deferring therapy, such as a better quality of life and less risk of developing resistance, and the main factor favoring initiation of therapy, which is avoidance of deterioration of the immune system to the point that it cannot be rescued with antiretroviral therapy. There are data that support earlier initiation of therapy than the recommendations above advise, such as the Wang study, which showed a higher mortality for people who were started on HAART later, and other evidence that will be factored into future recommendations. There will no doubt be modifications from time to time in the recommendations based on studies of measures of viral replication and immunological function, the availability of clinically useful resistence studies, and with increased convenience and lower toxicity of available therapies. Similarly, the recommendations for initial therapy for HIV have evolved over time, with the current regimens being a choice of a ritonavir-boosted protease inhibitor plus two NRTIs, or a nonnucleoside reverse transcriptase inhibitor plus two NRTIs. Previously recommended regimens, such as 4-drug regimens, 3-NRTI regimens, and single-drug regimens, are no longer considered optimal. - Nunh-huh 04:01, 14 Jun 2005 (UTC)
- Further to this, here's the current AIDS treatment guidelines from the US Department of Health and Human Services. From page 8:
- When should therapy be started in patients with established asymptomatic infection?
- The Panel reaffirms the desirability of initiating therapy before the CD4 cell count falls below 200 cells/mm3. In addition, there are inconsistent data documenting added value in treating before the count falls below 350 cell/mm3, but some clinicians opt to consider treatment in patients with CD4 count >350 cell/mm3 and HIV-RNA >100,000 copies/mL. A review of the literature on this issue can been seen in the When to Treat: Indications for Antiretroviral Therapy section.
- Like I said, the jury's still out on this. -- Robert Merkel 03:53, 14 Jun 2005 (UTC)
- Going back to the original point, there's not much directly on this in the guidelines but they do say the following, in regards to reasons for commencing therapy: "Potential Risks of Deferred Therapy include:...the increased risk for HIV transmission to others during a longer untreated period.". So these guys seem to think that antivirals can reduce the risk of HIV transmission, and that's a relevant factor for considering when to commence treatment. -- Robert Merkel 04:04, 14 Jun 2005 (UTC)
Alternative theories
The purpose of this section appears to be to ridicule some Nobel laureates and the Murdoch press, without actually stating their views. Words like, mainstream, activists, dissidents, and AIDS denialism are all emotive words, which judge positions that are not presented. I am deleting it Joe Merkel 02:34, 12 Jun 2005 (UTC)
Main article: AIDS reappraisal
A few scientists and AIDS activists continue to question the connection between HIV and AIDS, the very existence of HIV, or of an independent AIDS disease. The validity of current testing methods is also questioned. Dissident scientists report that they are usually not invited to attend AIDS conferences and are not granted research funding from most mainstream sources. Prominent members of this group are virus researcher Peter Duesberg and Nobel Prize laureate Kary Mullis. These theories have been in the field for at least 15 years, and have found little support beyond the original circle of advocates. They gained prominence when they were promoted, for reasons which have never been made clear, by sections of the Murdoch press, such as the Sunday Times and The Australian.
Dr. Robert E. Willner caught the attention of the Spanish media, when in 1994 he inoculated himself with the blood of Pedro Tocino, an HIV positive hemophiliac on live TV. Dr. Willner died of a [[heart attack]] in 1995.
Mainstream AIDS activists characterize the position of these dissidents as " AIDS denialism," and believe their public proselytization for their various theories is destructive to the adoption of appropriate preventive and therapeutic measures. Active advocacy of these theories is largely confined to radical gay activist groups such as ACT-UP in San Francisco. (Not to be confused with ACT-UP/Golden Gate, which split from ACT-UP San Francisco in 1990, and changed its name in 2000 to avoid association with ACT-UP/San Francisco's non-mainstream views). As with the enthusiasm for alternative therapies, advocacy of unorthodox views about AIDS has declined with the increasing success of orthodox medical approaches to AIDS therapies.
Origins edit
This is the AIDS article, so the first point is that "AIDS spread initially in West Africa." As this is the habitat of the common chimpanzee genetic comparisons of HIV and SIV were done by the team at University of Alabama. 1999 is the date of publication not when the research was done. The researchers have wisely avoid speculation about how the transfer from chimpanzee to human occured. Weiss, a leading expert in AIDS, suggests the butchering of chimpazees for meat is a possiblity. Beliefs about prostitutes are unsupported by evidence. The polio vaccine theory has also been investigated and discarded. An encyclopedia is not a repository of every discredited belief, blind alley or red herring. Stick to the facts than can be referenced.
The is no reason to repeat the artists impression of HIV. It is already on the HIV article. Joe Merkel 16:56, 12 Jun 2005 (UTC)
What is a section about the origins of HIV doing in the AIDS article? Is the correct place the HIV article. Sci guy 14:12, 13 Jun 2005 (UTC)
Treatments and vaccines edit
I have divided this into two sections, because treatments are for people with AIDS and vaccines are intended to prevent HIV - actually vacines probably belong in the HIV article.
I have edited to the 2002 treatment guidelines and linked to the Antiretroviral drug article. Statements like "The majority of the world's infected individuals, unfortunately, do not have access to medications and treatments for HIV and AIDS." are demeaning, racist, and inaccurate. The fact is the majority of the HIV infected people in the world do not meet the current treatment guidelines! Joe Merkel 17:05, 12 Jun 2005 (UTC)
Treatments and Vaccines.
Section excised until dispute solved. Please write alternate versions here, discuss and come to agreement. HINT: fact checking is good.-- Tznkai 16:17, 15 Jun 2005 (UTC)
Antiretroviral regimens are complex, have serious side effects, pose difficulty with adherence, and carry serious potential consequences from the development of viral resistance because of nonadherence to the drug regimen or suboptimal levels of antiretroviral agents. Patient education and involvement in therapeutic decisions are critical. Treatment should usually be offered to all patients with symptoms ascribed to HIV infection. Recommendations for offering antiretroviral therapy among asymptomatic patients require analysis of real and potential risks and benefits. Panel on Clinical Practices for Treatment of HIV. September 2002
There is ongoing research into developing a
vaccine for HIV and in developing new anti-retroviral drugs. Human trials are currently underway. Research to improve current treatments includes simplifying current drug regimens to improve adherence and in decreasing side effects.
VIRxSYS Corporation has developed an innovative HIV lentiviral vector, called VRX496, that can be used to combat the HIV virus. The method has entered Phase I clinical trials, and it is the first-ever use of a lentiviral vector in humans. If results are positive, the method might be proven an effective cure for the AIDS disease.
Ever since AIDS entered the public consciousness, various forms of alternative medicine have been used to treat its symptoms. In the first decade of the epidemic when no useful conventional treatment was available, a large number of PWAs experimented with alternative therapies of various kinds, including massage, herbal and flower remedies and acupuncture, to either combat the virus or to relieve related symptoms. None of these were shown to have any genuine or long-term effect on the virus in controlled trials, but they may have had other quality of life-enhancing effects on individual users. Interest in these therapies has declined over the past decade as conventional treatments have improved. They are still used by some people with AIDS who do not believe that HIV causes AIDS. Alternative therapies such as massage, acupuncture and herbal medicine are still used by many sufferers in conjunction with other treatments, mainly to treat symptoms such as pain and loss of appetite. People with AIDS, like people with other illnesses such as cancer, also sometimes use marijuana to treat pain, combat nausea and stimulate appetite.
Alternate version: Newer treatments, however, have played a part in delaying the onset of AIDS, on reducing the symptoms, and extending patients' life spans. Over the past decade the success of these anti-retroviral treatments in prolonging, and improving, the quality of life for people with AIDS has improved dramatically.
Current optimal treatment options consist of combinations ("cocktails") of two or more types of anti-retroviral agents such as two nucleoside analogue reverse transcriptase inhibitors (NRTIs), and a protease inhibitor or a non nucleoside reverse transcriptase inhibitor (NNRTI). Patients on such treatments have been known to repeatedly test "undetectable" (that is, negative) for HIV, but discontinuing therapy has thus far caused all such patients' viral loads to promptly increase. There is also concern with such regimens that drug resistance will eventually develop. In recent years the term HAART (highly-active anti-retroviral therapy) has been commonly used to describe this form of treatment. The majority of the world's infected individuals, unfortunately, do not have access to medications and treatments for HIV and AIDS.
There is ongoing research into developing a vaccine for HIV and in developing new anti-retroviral drugs. Human trials are currently underway. Research to improve current treatments includes simplifying current drug regimens to improve adherence and in decreasing side effects.
VIRxSYS Corporation has developed an innovative HIV lentiviral vector, called VRX496, that can be used to combat the HIV virus. The method has entered Phase I clinical trials, and it is the first-ever use of a lentiviral vector in humans. If results are positive, the method might be proven an effective cure for the AIDS disease.
Ever since AIDS entered the public consciousness, various forms of alternative medicine have been used to treat its symptoms. In the first decade of the epidemic when no useful conventional treatment was available, a large number of PWAs experimented with alternative therapies of various kinds, including massage, herbal and flower remedies and acupuncture, to either combat the virus or to relieve related symptoms. None of these were shown to have any genuine or long-term effect on the virus in controlled trials, but they may have had other quality of life-enhancing effects on individual users. Interest in these therapies has declined over the past decade as conventional treatments have improved. They are still used by some people with AIDS who do not believe that HIV causes AIDS. Alternative therapies such as massage, acupuncture and herbal medicine are still used by many sufferers in conjunction with other treatments, mainly to treat symptoms such as pain and loss of appetite. People with AIDS, like people with other illnesses such as cancer, also sometimes use marijuana to treat pain, combat nausea and stimulate appetite.
Responses:
- I don't think anything is to be gained by discussing with radical AIDS denialists like Sci Guy and Fred2005. Time and again we have patiently explained things to them and provided sources, yet they still delete any information about benefits of AIDS treatment while adding their bullshit claims such as "AIDS is completely confined to gays and drug users in the US". I'm curious why you cut and pasted the AIDS denialist version of the section here, as opposed to the scientific consensus version. You don't get it, this isn't a legitimate dispute. It's the overwhelming scientific consensus versus a few fringe activists. Rhobite 16:36, Jun 15, 2005 (UTC)
- You're right. I don't get it because I'm not a scietist myself, and I don't magically know what the consensus is. I'm not here to cry what is true, but I do know when something needs discussion and when something doesn't. Alternate version is now up.-- Tznkai 16:55, 15 Jun 2005 (UTC)
September 2003 treatment guideline from Body
This link was in the references. Is it one of the AIDS denialist websites? They seem to be pushing the same line about defering treatment. [1]
- Doctors still disagree about when is the best time to begin HIV treatment, also called anti-retroviral therapy. You and your doctor will need to determine this together, but there are some respected guidelines. Be aware that these guidelines are regularly updated and are just suggestions based on the most recent research, and are not hard and fast rules.
- For example, the U.S. government's Department of Health and Human Services recommends that you begin HIV treatment if you have any serious symptoms, or if your T-cell count falls below 200. When your T-cell count drops below 200, you risk possibly irreversible health problems both before and after you begin treatment
Current Guidelines Recommend
- If your T-cell count is 350 or above, do not start medications unless your viral load is 55,000 or higher.
- If your T-cell count is between 200-349, treatment should be considered.
- If your T-cell count is below 200, treatment is indicated.
If the U.S. government's Department of Health and Human Services says do not do not start medications, if your T-cell count is 350 or above unless your viral load is 55,000 or higher - then who is advocating early treatment?
As editors it is our role to source the facts. Joe Merkel 15:08, 16 Jun 2005 (UTC)
- Considering treatment when CD4 count is between 200-350 is the current consensus in the various guidelines. Unfortunately, denialists like you look at any change in medical consensus as conclusive proof that doctors don't know what they're talking about. I have one more bone to pick with your edits: You added the text "Many people believe that newer treatments have played a part in delaying the onset of AIDS, on reducing the symptoms, and extending patients' life spans, although experts describe the data as inconclusive". I see that the word "inconclusive" came from the treatment pocket guidelines. The guidelines merely say that the data is inconclusive about whether to start treatment when CD4+ is above 350. You, however, made a misrepresentation (hopefully not deliberate) and claimed that the pocket reference guide was stating that the overall efficacy of HAART was "inconclusive". Hopefully this misrepresentation will stop, as I've linked to two large studies which show that HAART is effective, and which carry much more weight than a pocket treatment card. Rhobite 16:20, Jun 16, 2005 (UTC)
Aids and homosexuality
I think its important to talk about this, because atleast in the united states, there is a link in peoples minds, and there is a statistical link that it happens fairly often. Any takers?-- Tznkai 19:32, 13 Jun 2005 (UTC)
- There's no MEDICAL link, so I don't see your point, unless statistics is enough for you, in that case there's also a statistical link between the number of people with IQs below 100 and the number of conservative christians in this country,
- coincidence??
-any takers?-- 172.152.58.17 19:38, 13 Jun 2005 (UTC)
- Its important because this isn't a medical textbook, its an encylcopedia, and not putting the information in here leaves people trying to decide if Fred Phelps knows what he's talking about without a resource that leads them quickly to evidence to the contrary.-- Tznkai 19:49, 13 Jun 2005 (UTC)
- As I stated above, I think a summary of all the statistics put in laymens terms in it's own section of this document that publishes all the relevant data without singling out a particular minority for special notice would be the most balanced and neutral way of presenting this information and would still allow people to decide if Fred Phelps knows what he is talking about, without actually pandering to anyone's prejudices.
Axon 14:16, 14 Jun 2005 (UTC)
- Sounds good to me. Where would it go?-- Tznkai 16:58, 15 Jun 2005 (UTC)
- As I stated above, I think a summary of all the statistics put in laymens terms in it's own section of this document that publishes all the relevant data without singling out a particular minority for special notice would be the most balanced and neutral way of presenting this information and would still allow people to decide if Fred Phelps knows what he is talking about, without actually pandering to anyone's prejudices.
Axon 14:16, 14 Jun 2005 (UTC)
In the United States, 75% or reported AIDS cases were attributed to male-to-male sexual contact or injection drug use. These are the two original risk groups identified in 1983, before HIV blood screening was available. This is very different from Africa. I consider "male-to-male sexual contact or injection drug use" to be a NPOV description of behaviour Sci guy 03:01, 14 Jun 2005 (UTC)
- Sci-guy, that statistic is completly out of context. Reading through the talk history I can see that it came out of a legitimate attempt to neutralize an inserted statistic, but it equivocates malemale and drug users!-- Tznkai 13:54, 14 Jun 2005 (UTC)
Fred2005's nonsense
This article is getting torn up by Fred's edits. He is replacing well-written paragraphs with dire warnings about the dangers of HIV treatment and claims of controversy about early treatment. Of course we should mention the most current guidelines for starting treatment, but in a neutral manner (and without removing information on the benefits of HAART). Rhobite 16:33, Jun 14, 2005 (UTC)
- I believe Fred2005 has broken the 3RR rule [2] [3] [4] [5] with his last edit. Axon 16:39, 14 Jun 2005 (UTC)
Removal of talk page comments
Uh, where did my remarks on this talk page go? It seems they have been completely deleted by SciGuy [6]. They are not in the talk archives or the NPOV dispute branch SciGuy created. Axon 16:42, 15 Jun 2005 (UTC)
What has happened here??
A couple of weeks ago this article was great. It was comprehensive, well written, flowed well... Now it's a mess. The writing is terrible, relevant information has been cut, the flow is off... What's going on? Exploding Boy 17:10, Jun 15, 2005 (UTC)
- It has been invaded by the POV warriors. The stench of POV is terrible. I think it is time for an RFM on some editors who remove valid information to suit their views.
JFW |
T@lk 18:04, 15 Jun 2005 (UTC)
- What he said. →Raul654 18:06, Jun 15, 2005 (UTC)
- I think it would be a good idea if someone creates a sub-page here with an older, un-POV'd version of this article and calls for a RfC. Axon 18:07, 15 Jun 2005 (UTC)
- I'm vaugley new. You mean this article was ok once upon a time? From where I started, I lost track of what the facts were since no one does any fact checking around here -- Tznkai 18:12, 15 Jun 2005 (UTC)
- According to ExplodingBoy it was: any comments ExplodingBoy? Axon 18:16, 15 Jun 2005 (UTC)
- Mediation.. I wish I was as patient as you guys. I don't think this will stop until editors like Sci Guy and Fred2005 are banned from editing AIDS-related articles. Rhobite 18:14, Jun 15, 2005 (UTC)
I've reverted to EB's version from May 18 (with a few tweaks to incorperate the new pictures and remove the depricated lists). →Raul654 19:01, Jun 15, 2005 (UTC)
- Fabulous. I was stunned at first over the massive rollback, and reasserted the NPOV flag, but once I read it, I reverted my flag. It's pretty darn good. Whig 19:45, 15 Jun 2005 (UTC)
- Unfortunately some of Sci Guy's stuff is left in the article, e.g. the "AIDS is defined as occuring" gibberish, direct out of context quotes from random NIH reports (passed off as Sci Guy's own words), Bangui definition, etc. Still needs some work but overall this version is better than the one from the past few days. Rhobite 20:39, Jun 15, 2005 (UTC)
- The Bangui definition and discrepancy with HIV antibodies should not be in the intro. A number of tropical illnesses or combinations thereof could easily fulfil the Bangui criteria, fuelling Sci Guy's nonsense about discrepancy between clinical and laboratory AIDS.
- It should be mentioned that Koch's postulates have been met hundreds of times over for AIDS, confirming HIV as an agent and effectively relegating the Duesberg psychos to the history of medicine. JFW | T@lk 20:46, 15 Jun 2005 (UTC)
- I agree that the Bangui def is out of place in the intro, but it is definitely significant for a history section or "History of AIDS" article IMHO.
- As for the Koch's postulates argument... well, yes, that's also worth a mention, but I just know there's a POV battle looming if we use it to clobber alternate hypotheses. - jredmond 21:03, 15 Jun 2005 (UTC)
- Of course the Bangui def should be here, just in the history section. As for Koch's postulates, we should mention which study first fulfilled them; this the bread & butter of clinical microbiology. JFW | T@lk 22:34, 15 Jun 2005 (UTC)
- Any chance that that study (or at least an abstract thereof) would be online? As long as we even imply that there's a connection between HIV and AIDS, we'll have POV warriors coming through, but a link to a peer-reviewed study should dramatically reduce their number and severity. - jredmond 22:57, 15 Jun 2005 (UTC)
- PMID 8902385 mentions it, but I can't find the studies it refers to. I'll go through the article and come back to this page. Here is something more interesting. JFW | T@lk 23:48, 15 Jun 2005 (UTC)
- I do like the second one better... but hell, let's link 'em both. - jredmond 23:58, 15 Jun 2005 (UTC)
- Sounds like a good idea--but be forewarned: peer-reviewd studies don't seem to do much good in convincing idealogues of scientific evidence. Carl Henderson 23:46, 15 Jun 2005 (UTC)
- I know. But it's pretty tough to mess with links to peer-reviewed studies without raising a lot of vandal/POV warrior flags and attracting a whole lot of negative attention. - jredmond 23:58, 15 Jun 2005 (UTC)
- Thanks for remembering the images. I went back in and adjusted the image sizes. The "HIV Daughter Particles" image was sized at higher than its native resolution. I also upsized the "HIV Viron" image so that all the the text could be read (at least on my screen). Carl Henderson 23:46, 15 Jun 2005 (UTC)
Oh yeah. That's more like it. Exploding Boy 00:55, Jun 16, 2005 (UTC)
I think this statement needs to be reworded for NPOV: "The situation in South Africa, where President Thabo Mbeki shares the beliefs of "AIDS denialists," is a negative influence and neglection of the fact that 4.7 million infections took place for 2002." Whig 03:04, 16 Jun 2005 (UTC)
Japan's tainted blood scandal
Please see [7]. Exploding Boy 02:24, Jun 16, 2005 (UTC)
- One of the most famous hemophilia patients was Stephen Christmas, namesake of Christmas disease. He is a case in point. JFW | T@lk 15:42, 16 Jun 2005 (UTC)
- Yes... but he's not Japanese and he wasn't a part of the Japanese tainted blood scandal... I"m really looking for imput on how to title the article or where to find it if one already exists. Exploding Boy 18:44, Jun 20, 2005 (UTC)
Please see HIV-tainted blood scandal (Japan). Exploding Boy 00:51, Jun 21, 2005 (UTC)
undetectable
I have a problem with:
"Patients on such treatments have been known to repeatedly test "undetectable" (that is, negative) for HIV, but discontinuing therapy has thus far caused all such patients' viral loads to promptly increase"
Does "have been known" mean that this is an unusual or rare outcome?
I assume the intention is to claim that viral load blood test is undetectable rather suggesting that such treatments mean a person is negative for HIV on the antibody test.
I suggest we need a source reference so we can edit this to avoid misunderstanding Joe Merkel 15:33, 16 Jun 2005 (UTC)
- No, antibodies persist. Viral load has a lower limit of detection, and the virus may be reactivated if HAART is stopped. There is nothing counterintuitive about this, and may not even need sourcing. Antiretrovirals suppress viral replication, sometimes to the point that the viral load is under the detection limit, but when discontinued the virus comes back. Sure. JFW | T@lk 15:40, 16 Jun 2005 (UTC)
Joe, I am sick of people coming in to the treatment section and "nerfing" it with vague phrases like "Many people believe that newer treatments have played a part in delaying the onset of AIDS". Peer-reviewed research and clinical trials should not be described as "many people". Many times over, studies have showed that patients who properly adhere to therapy have much lower viral loads, higher CD4 counts, and longer survival times. I am linking to two of these studies so please cut out the vague rewrites. [8] [9]
Also, please stop mentioning the dangers of antiretroviral therapy before it is even described. HAART is not perfect. I'm not trying to hide mention of these problems, but mentioning them before HAART is even described is confusing and dismissive. Rhobite 16:01, Jun 16, 2005 (UTC)
- Rhobite, could you cite PMID abstracts scientifically in a section called "References" and using footnotes? This massively improves the credibility of your edits. See obesity for an example. JFW | T@lk 16:22, 16 Jun 2005 (UTC)
- The automatic footnoting system is currently a huge pain to work with, due to the lack of automatic renumbering. With the article under attack by people who don't mind removing references, I think using the system would be futile. I will add them as general references with no footnotes, however. Rhobite 16:44, Jun 16, 2005 (UTC)
- Rhobite, new users don't know how to properly refrence. You do. Show a better example.-- Tznkai 16:49, 16 Jun 2005 (UTC)
- I just added a references section. If that isn't good enough for you, feel free to implement automatic footnoting. As you've only been around here for a couple weeks you may not yet realize that automatic footnotes are close to impossible to maintain in a rapidly changing article such as this one. As I said, I'm not being lazy, I think using automatic footnotes would be futile right now.
- I prefer to spend my time on this article refuting fringe opinions about AIDS, as opposed to constantly reordering footnotes. How you choose to spend your time is your business. I'd appreciate fewer patronizing remarks, and more beneficial contributions out of you. Rhobite 17:03, Jun 16, 2005 (UTC)
- Good call on the named references, I will add those to the treatment section. Rhobite 18:39, Jun 16, 2005 (UTC)
Liver Failure
Under paragraph two of "AIDS epidemic," the article currently states, "In the United States, the most common cause of death for people with AIDS is liver failure caused by antiretroviral drugs." I'm very skeptical of this statement--especially considering many people with AIDS in the US are also co-infected with Hepatitis B or C.
The only source I can find for the liver failure mortality claim is a University of Pittsburgh Medical Center press release [10] highlighting a study by Dr. Amy Justice, presented at 14th International AIDS Conference in Barcelona (2002). She is quoted, saying, "[f]urthermore, the fact that the most common current cause of death among people with HIV is liver failure suggests that liver injury may be a major limiting factor in the effectiveness of current HIV treatment." That quote was then picked up in several news articles and ended up on lots of the "HIV doesn't cause AIDS" websites.
Can anyone verify that liver failure caused by antiretroviral drugs is the most common cause of death for people with AIDS in the US? I tried, and I can't. Carl Henderson 00:14, 17 Jun 2005 (UTC)
- In any case, even if antiretrovirals do ultimately end up killing people through liver failure, it doesn't necessarily follow that antiretroviral treatment is bad; AIDS may well have killed them sooner and more painfully...-- Robert Merkel 03:08, 17 Jun 2005 (UTC)
- Shouldn't matter, we just need the facts, right?-- Tznkai 03:19, 17 Jun 2005 (UTC)
- As long as they're presented accurately and neutrally. Some people have a tendency to put the cart before the horse when describing the negative aspects of antiretroviral drugs. Rhobite 03:33, Jun 17, 2005 (UTC)
- My point is I don't think "most common current cause of death among people with HIV is liver failure" is "the facts." I've only found one primary reference to it--and that was a press release--not the original study cited. I'm looking for some more sources one way or another.
- Nevertheless, the way the article currently phrases the "liver failure" claim is wrong. With the widespread co-infection of Hepatitis B or C among many groups of AIDS patients in the US, it would be impossible to ascribe all deaths from liver failure to antiretrovirals. Carl Henderson 15:14, 17 Jun 2005 (UTC)
- Whether retrovirals are "good" or "bad" isn't a judgment that Wikipedia can make. We can and should cite references showing their effects on mortality rates from AIDS as well as from direct toxicity. I think that any reasonable person would hope that less toxic effective treatments would eventually be found, we ought not to sanitize the effects (positive or negative) from AZT and HAART, etc. Whig 03:49, 17 Jun 2005 (UTC)
It's certainly not true that "liver failure caused by antiretroviral drugs" is the leading cause of death in HIV infected people in the U.S. And we have no citation for that assertion. I suspect what's happened is someone has taken a study in which the most common cause of non-AIDS-related death in AIDS patients is liver failure, added their erroneous assumption that this was due to drugs rather than co-infection with hepatitis B or C, and asserted it here as fact. One study showing results capable of such misinterpretation (but in France rather than the U.S.) is here, and another one among women here. In all such studies, liver failure remains one of the more common types of non-AIDS-related deaths, but non-AIDS-related deaths are dwarfed by AIDS-related causes. A possible explanation of the high incidence of renal and hepatic failure is suggested here to be a rising proportion of drug addict in the population. But we shouldn't be misinterpreting all liver failure in the HIV infected as drug-induced. - Nunh-huh 21:41, 17 Jun 2005 (UTC)
- I've been doing some research and have now found studies both confirming and disconfirming the "In the United States, the most common cause of death for people with AIDS is liver failure" part of the statement, but not the "caused by antiretroviral drugs" clause. Note that I've included references to two studies looking at the Mortality 2000 study group in France. I'm assuming that the demographics of AIDS patients in France are not that different from those in the US.
- First the disconfirming studies:
- Changes in Mortality Related to Human Immunodeficiency Virus Infection: Comparative Analysis of Inpatient Deaths in 1995 and in 1999–2000
- Clinical Infectious Diseases, 2003;36:1030-1038
- Mamta K. Jain, Daniel J. Skiest, Jeff W. Cloud, Charu L. Jain, Dennis Burns, and Ruth E. Berggren
- ABSTRACT: We conducted a retrospective chart review of human immunodeficiency virus (HIV)–infected patients who died in 1995 and in 1999–2000. We found an increase in the proportion of patients who died from an illness that was not related to acquired immunodeficiency syndrome (AIDS). Although there was a decrease in the prevalence of AIDS-defining illnesses, >85% of patients died with CD4 counts of <200 cells/μL. The leading cause of death was Pneumocystis carinii pneumonia (PCP). Nonadherence to therapy and new diagnosis of HIV infection were the leading reasons why patients were not receiving antiretroviral therapy. The leading causes of non–AIDS-related deaths in 1999–2000 were non–AIDS-defining infections and end-stage liver disease. At our hospital, PCP remains an important cause of death in the highly active antiretroviral therapy (HAART) era, possibly because >50% of HIV-infected patients who died were not receiving HAART. AIDS-defining illnesses continue to be a major cause of mortality in the HAART era in populations where access to care and adherence to HAART is limited.
- Causes of death among human immunodeficiency virus (HIV)-infected adults in the era of potent antiretroviral therapy: emerging role of hepatitis and cancers, persistent role of AIDS
- International Journal of Epidemiology, 2005 Feb;34(1):130-1.
- Lewden C, Salmon D, Morlat P, Bevilacqua S, Jougla E, Bonnet F, Heripret L, Costagliola D, May T, Chene G; Mortality 2000 study group
- ABSTRACT: Background-In the era of highly active antiretroviral therapy (HAART) mortality has decreased substantially among human immunodeficiency virus (HIV)-infected people with access to HAART, but there are concerns regarding co-morbidities and adverse effects of HAART, which may impair vital prognosis. The Mortality 2000 study examined the causes of death in HIV-infected adults at a national level in France in the year 2000. Methods-All French hospital wards known to be involved in the management of HIV infection were asked to notify prospectively the deaths that occurred in 2000 among HIV-infected adults. The causes of death were documented using a standardized questionnaire. Results-The 185 participating wards notified 964 deaths. The main underlying causes of death were AIDS-related (47%, non-Hodgkin's lymphoma: 23%), viral hepatitis (11%, hepatitis C: 9%, hepatitis B: 2%), cancer not related to AIDS or hepatitis (11%), cardiovascular disease (7%), bacterial infections (6%), suicide (4%), and adverse effect of antiretroviral treatments (1%). Among AIDS-related deaths, HIV infection had been diagnosed recently in 20%. Smoking was recorded in 72% of cancer-related deaths and alcohol consumption in 54% of hepatitis-related deaths. Among non-HIV related deaths between 25 and 64 years, the proportion of infectious diseases (including HCV and HBV-related deaths) was higher in HIV-infected adults than in the general population. Conclusions-Improved strategies for detecting HIV infection before AIDS-defining complications occur are needed in the era of HAART. The prevention of non-AIDS related cancers, especially lung cancer, the management of non-Hodgkin's lymphoma, and of viral hepatitis are also important priorities.
- Causes and characteristics of death among HIV-1 infected patients with immunovirologic response to antiretroviral treatment
- Presse Medicale,. 2004 Dec 4;33(21):1487-92.
- May T, Lewden C Bonnet F, Heripret L, Bevilacqua S, Jougla E, Costagliola D, Morlat P, Salmon D, Chene G; Groupe d'Etude Mortalite 2000
- ABSTRACT: To analyse the causes of death among HIV-infected adults in France in the year 2000. METHODS: Based on data from a national survey, our study describes and analyses the causes and characteristics of patients with immunological and virological response (CD4>200/mm3, ARN-HIV<500 copies/mL), who died during antiretroviral treatment. RESULTS: Among a total of 964 deaths registered, data on 864 cases were available for analysis. One hundred forty-nine patients (17%)were immunovirological responders. The underlying causes of death were non AIDS-defining malignancies for 36 (24%), mainly due to lung cancer (16 cases), hepatocarcinoma (7) and ano-rectal carcinoma (3), AIDS for 22 (15%), mainly due to Non Hodgkin Lymphoma (10 cases) and uterine cancer (3), cardiovascular diseases for 22 (15%), post hepatitis C hepatic failure for 16 (11%), suicide for 16 (11%), and bacterial infections for 14(9%). When comparing characteristics of death in the 149 responders versus the 715 other patients, the responders were significantly more frequently: co-infected by HCV+ (45 vs. 33%), injected drug addicts (40 vs. 27%),alcoholics (38 vs. 28 %), and dyslipidemics (19 vs. 11%). In 2000,around 20% of registered deaths of HIV patients in France had occurred among good immunovirological responders. CONCLUSION: To further reduce mortality among such efficiently treated patients, attention must be focused on treatable conditions such as hepatitis C, dyslipidemia and on the prevention of malignancies such as lung cancer and cervical or ano-rectal carcinoma.
- (abstract only--article in French)
- Now for a confirming study:
- Increasing Mortality Due to End-Stage Liver Disease in Patients with Human Immunodeficiency Virus Infection
- Clinical Infectious Diseases, 2001;32:492-497
- Ioana Bica, Barbara McGovern, Rakesh Dhar, David Stone, Katherine McGowan, Rochelle Scheib, and David R. Snydman
- ABSTRACT: Highly active antiretroviral therapy has decreased human immunodeficiency virus (HIV)–associated mortality; other comorbidities, such as chronic liver disease, are assuming greater importance. We retrospectively examined the causes of death of HIV-seropositive patients at our institution in 1991, 1996, and 1998–1999. In 1998–1999, 11 (50%) of 22 deaths were due to end-stage liver disease, compared with 3 (11.5%) of 26 in 1991 and 5 (13.9%) of 36 in 1996 (P = .003). In 1998–1999, 55% of patients had nondetectable plasma HIV RNA levels and/or CD4 cell counts of >200 cells/mm3 within the year before death. Most of the patients that were tested had detectable antibodies to hepatitis C virus (75% of patients who died in 1991, 57.7% who died in 1996, and 93.8% who died in 1998–1999; P = NS). In 1998–1999, 7 patients (31.8%) discontinued antiretroviral therapy because of hepatotoxicity, compared with 0 in 1991 and 2 (5.6%) in 1996. End-stage liver disease is now the leading cause of death in our hospitalized HIV-seropositive population.
- Plus a link to a Powerpoint presentation citing several studies (that I've not had a chance to run down) also supporting the "liver failure" claim:
- Liver disease has emerged as a major cause of mortality in the HAART era.
- http://www.roche-hiv.com/roche-in-hiv/Conferences/Documents/02-Dieterich-Show.ppt
- My conclusion--I don't think the research firmly supports the "liver failure" claim, but I also don't think I'm qualified to make any such conclusion as far as Wikipedia is concerned.
- Help. Carl Henderson 05:40, 18 Jun 2005 (UTC)
"AIDS results from..."
This may have been discussed before, but does anyone think the sentence at the top
"AIDS results from an infection of HIV, the Human Immunodeficiency Virus, although some debate this."
is really poor? I mean, the first part says - "HIV results in AIDS" and the second - "It's debatable that HIV results in AIDS". Can't we say something like "AIDS results from an infection of HIV, the Human Immunodeficiency Virus. Though the later has been widely credited, some still debate the origin of AIDS." Or maybe even take out "although some debate this." all together from the beginning and add it as a counter-point later in the article. Having it in the intro just makes a weak impression for the everything else. JoeSmack (talk) 15:32, Jun 17, 2005 (UTC)
I have never had a problem with "HIV causes AIDS". It is the same as "smoking causes lung cancer" or "speeding causes road accidents". The October 2004 version from U.S. Department of Health and Human Services is as follows:
- A positive HIV test result means that you are infected with HIV (Human Immunodeficiency Virus), the virus that causes AIDS (Acquired Immune Deficiency Syndrome). Being infected with HIV does not mean that you have AIDS right now. However, if left untreated, HIV infection damages a person’s immune system and can progress to AIDS. [11]
I was surprised by the "can" in "HIV infection damages a person’s immune system and can progress to AIDS". But the issue is not what you or believe, we are editors searching for facts that can be verified. So I agree with you that "although some debate this." is really poor. Who debates this? On what basis? When? As we are reminded each time we edit - "Please cite your sources so others can check your work." Sci guy 16:31, 17 Jun 2005 (UTC)
- I'm not sure how much more factual you can get than U.S. Department of Health and Human Services.
JoeSmack
(talk) 16:36, Jun 17, 2005 (UTC)
- The UN? I think Sci guy was referring to the "debate on this" part.-- Tznkai 16:40, 17 Jun 2005 (UTC)
- and the reason that "can" is in there is because of long-term HIV nonprogressors - HIV does lead to AIDS for a vast vast majority of those infected when left untreated. JoeSmack (talk) 16:41, Jun 17, 2005 (UTC)
I have removed the offending phrase (which I wrote in the first place). →Raul654 17:18, Jun 17, 2005 (UTC)
Major changes
Alright guys, don't be scared, but I printed this thing out and started using a red pen. Mostly it has been removing things stated as facts that have no cite, things that don't belong in the article (the prevention section has a stupidly long thing on company condom testing), and things that should be moved. I am doing it in sections so that people can see the changes more easily.
I've gotten about halfway through the article with the red pen, and will finish and add the last half after i change the first half on here. Feel free to talk about the changes. JoeSmack (talk) 17:29, Jun 17, 2005 (UTC)
- i reverted one part where breastmilk etc. was deleted from the prevention section. it is really important info but it has no cite. please please someone find one and put it in so we can use it. JoeSmack (talk) 18:02, Jun 17, 2005 (UTC)
man, WTF guys? anyone notice that the Origin of AIDS section, probably one of the most important, has NO CITES whatsoever? you guys are telling me there is no book on the history of AIDS out there? -- someone please take this one on, i'm not even going to touch it cause i'd just delete the whole thing (important yes, but there are no cites). JoeSmack (talk) 18:12, Jun 17, 2005 (UTC)
- the Current medical understanding of AIDS section is just no cite after no cite. They just state them like they are facts or says 'studies have shown'. This is depressing guys, i'm not touching this thing either. JoeSmack (talk) 18:17, Jun 17, 2005 (UTC)
about that "devistating" remove. 23 million people in 24 years. imagine in 24 years from now you went to washington. everyone there would be dead. went to utah, everyone there would be dead. nevada. oregon. north dakota, nebraska.... doesn't that seem devistating? am i pushing the line with that word? JoeSmack (talk) 18:22, Jun 17, 2005 (UTC)
alright, I cant stand this ridiculas lack of citing sources. i'm stopping and continuing tomorrow or something. i'll be around if anyone wants to talk about the changes i've already made. JoeSmack (talk) 18:26, Jun 17, 2005 (UTC)
- Of course I agree with you, it is devastating. But it's POV for the article to use such words, even if most people would agree with them. The word doesn't enhance the sentence at all, it's just an appeal to emotion.
- About removing uncited parts. I agree that many parts of this article need citations. I don't know if the proper response is to simply remove them. Assuming that most of the contributions were made in good faith, I think it might be better to leave them in the article for the time being, and make a list of these claims which need to be cited. Then we can simply check things off the list once they are verified. Whether we leave them in the article or remove them, I think we need a list of uncited claims. People tend to forget about text once it's removed from an article, so we should keep track of these claims with the intention of replacing them. Would you be interested in helping to make this list?
Rhobite 18:34, Jun 17, 2005 (UTC)
- if you leave uncited parts until they are verified it can only cause problems. for instance, "AIDS has been correlated in men between 21 and 31 to higher speeding practices in cars." -- I made that up, it's bullshit. People who spread misinformation about AIDS do dumb stuff like this all the time, and to leave it there would be a disservice to people trying to educate themselves on AIDS everywhere. We shouldn't selectively decide 'which are probably true' and which aren't, so I think the best solution right now is to delete them.
Facts sourced
Alrighty guys, i added sources for the 1 in 200 rate of HIV infect for a needle prick and prevention for mothers birthing and breastfeeding for infants. Any takers for other sourceless facts? I've got list of removed 'facts' on my talk page that just need sources to go back in... JoeSmack (talk) 21:43, Jun 17, 2005 (UTC)
- I'm working on the "liver failure" claim. I'll also check the "[i]n Africa, the most common cause of death for people with AIDS is Tuberculosis" while I'm at it. I'll see if I can run down some of the others while I'm researching those, too. Carl Henderson 22:15, 17 Jun 2005 (UTC)
- I've done some research on the "liver failure" assertion, and posted it above under the Liver Failure section in the talk. Carl Henderson 05:42, 18 Jun 2005 (UTC)
- Here's another factoid sourced to add to the list. A previous version of the article stated that "Blood tranfusions remain a major source of new HIV infections worldwide. WHO estimated in 2000, between 15% and 20% of new HIV infections worldwide were the result of blood transfusions, where the donors were not screened or inadequately screened for HIV."
- Not quite accurate. According to a 2000 WHO press release Blood Safety... For Too Few, "between 5% and 10% of HIV infections worldwide are transmitted through the transfusion of infected blood and blood products. WHO/UNAIDS estimate that 5.6 million new HIV infections occur annually." This number is consistant with the WHO Global Database on Blood Safety's Summary Report for 1999-1998 which estimates that 43% of the blood supply in developing nations is not screened for HIV or other blood transmissible infections.
- Carl Henderson 00:52, 20 Jun 2005 (UTC)
- More cites found:
- "Chances of HIV transmission from infected male to female in a single act of genital sex are quite low: it is estimated that under normal conditions, only about 1 in 1000 acts results in infection." and "Transmission of virus from females to males is even less likely, but still possible."
- Acording to the CDC table SciGuy added Friday, these numbers are correct. I'd suggest a rewrite to say something like, "According to the CDC estimates (reference the table here), chances of HIV transmission from infected male to female in a single act of unprotected genital sex are quite low; it is estimated that under normal conditions, only about 10 in 10,000 acts results in infection. Transmission of virus from females to males is only about half as likely--though still possible. Note that these CDC estimates are averages, and actual odds of transmission of HIV via a single sexual act can be affected by other factors, such as the viral load of the infected partner or the presence of abrasions or sores on the genitals of either of the sexual partners." And if this section is rewritten, it should also be made clear that the CDC figures are based on AIDS in America, and that the methods of transmission elsewhere may not show the same pattern.
- One other thing. Factors such as drug use and the presence of other sexually transmitted diseases can also increase the likelyhood of transmission of HIV. Carl Henderson 18:24, 20 Jun 2005 (UTC)
- "One study concluded that 7.8% of recently infected men in San Francisco were probably infected through oral sex."
- Dillon B, Hecht FM, Swanson M et al., Primary HIV infections associated with oral transmission, 7th Conference on Retroviruses and Opportunistic Infections, San Francisco, January 30th-February 2nd, 2000 (abstract 473).
- That single 2000 study doesn't tell the whole story, though. The Public Health Agency of Canada has a good (and refenced) summary of various studies concerning oral HIV transmission, Oral Sex and the Risk of HIV Transmission. Research summarized in that May 2004 article demonstrated a wide range of risk estimates. Studies of different cohorts of homosexual males showed that from 3.9% to 16.2% were infected via receptive oral intercourse. Studies of different cohorts of hetrosexual couples showed that anywhere from 0% to 6.7% of heterosexual females were infected via receptive oral intercourse. Finally the PHAC article the overall literature, and found, "exposure to HIV through unprotected oral intercourse as an independent risk factor for HIV acquisition in only three (12.5%) of 24 epidemiological studies designed to examine risk of HIV from different sexual exposures."
- "A study of Spanish men who knowingly engaged in oral sex with HIV+ partners identified no cases of oral transmission."
- Evaluating the risk of HIV transmission through unprotected orogenital sex, Del Romero J, Marincovich B, Castilla J et al., AIDS 2002;16(9): 1296-97. Note that the study doesn't just concern Spanish men; the article covers a cohort of "135 seronegative individuals (110 women and 25 men), whose only risk exposure to HIV was unprotected orogenital sex with their infected partner."
- Carl Henderson 18:20, 20 Jun 2005 (UTC)
Why the heck has Bangui worked its way back in?
I thought I'd dealt with the Bangui definition way back in this edit. Why has this complete red herring, complete with unsourced claims about half the AIDS cases in Africa, snuck its way back into the article? -- Robert Merkel 08:45, 19 Jun 2005 (UTC)
I agree. The 'Bangui definition' is not part of the current definition, neither is hemophilia, Haitian, or male homosexual. The current definition based on HIV antibodies, T cells and AIDS defining illnesses would be better. Sci guy 14:12, 19 Jun 2005 (UTC)
- For those new to this article, Sci guy was the major proponent of the "Bangui definition" stuff in the first place. Please stop playing games. -- Robert Merkel 01:43, 20 Jun 2005 (UTC)
- Yes, he has changed tactics. Now he simply cuts and pastes selected bits of CDC literature into the article, in an effort to decrease readability I guess. Rhobite 02:01, Jun 20, 2005 (UTC)
Africans & genetics
I have heard that Africans are more likely to contract AIDS due to genetic factors and that a minority of those with Scandinavian genes are immune to it. Perhaps we should include something about this? 207.224.198.170 16:50, 19 Jun 2005 (UTC)
- You're thinking of the CCR5-Delta32 mutation, which provides some protection against HIV infection and is more common in those of European descent. see the CCR5 page in OMIM or do a Medline search on "CCR5-Delta32". - Nunh-huh 05:14, 20 Jun 2005 (UTC)
Drowning in statistics and terminology
I'm assuming that Sci guy's new tactic is simply to drown readers in overwhelming statistics and impenetrable language, such as the new CDC graphic and the large lists of people infected per region and deaths per region. I'm not saying this data shouldn't be in there, but there seems to be an intentional campaign to (a) make it take up as much space as possible and (b) copy complex language directly from medical studies.
For example, we just rewrote the lead section by hand over the past few days. I think the new lead is pretty good. Sci guy replaced the lead section with this text, copied directly from the CDC's MMWR, a publication which is intended for medical professionals:
- "The etiologic agent of acquired immunodeficiency syndrome AIDS is a retrovirus designated human immunodeficiency virus HIV. The CD4+ T-lymphocyte is the primary target for HIV infection because of the affinity of the virus for the CD4 surface marker. The CD4+ T-lymphocyte coordinates a number of important immunologic functions, and a loss of these functions results in progressive impairment of the immune response."
This text is basically unreadable to a layperson. I'm concerned that now that the legitimate contributors are making an effort to cite sources, Sci guy has shifted tactics towards trying to make the article as unreadable as possible. Sci guy please use your own words. Other people have taken the time to do research and write in language that is comfortable to read. If you are not willing or capable of doing the same, I'd ask that you please stop editing this article. All of your recent edits have been simple cut and paste jobs. Rhobite 16:57, Jun 19, 2005 (UTC)
- If you check the archive, you will find that Sci guy was previously criticized for NOT including the statement "The etiologic agent of acquired immunodeficiency syndrome AIDS is a retrovirus designated human immunodeficiency virus HIV." Now he is being criticized for including it! Is this article intended to contain, current referenced facts - or readable misinformation? For example the lead section now contains the popular misconception that "AIDS is a disease characterized by the destruction of the human immune system." In fact it is only part of the immune system the CD4 T cells that are affected, and this is thought to result in a loss of cell mediated immunity, and therefore vulnerablity to certain specifc diseases and some cancers. The current focus of AIDS is the heterosexaul epidemic in sub Saharan Africa. Fred2005 11:27, 20 Jun 2005 (UTC)
- Fred, you are quoting out of context. At the time, Rhobite was making the point that Sci Guy was selectively quoting the CDC (and back then, we were making the point that the article was unreadable through his and your efforts). Now, as Rhobite said, Sci Guy has switched gear to swamping the article in medical jargon. As to "destruction of the immune system", that's a good enough approximation for an article introduction. Now, stop wasting our time, please. -- Robert Merkel 12:34, 20 Jun 2005 (UTC)
| This page is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |