| This is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 |
Misdiagnosis Article at WHA
I was researching cluster headaches and I found Vast Majority of Cluster Headache Patients Are Initially Misdiagnosed. In short it says that most doctors were unable to properly identify cluster headache in the majority of patients. Some were led to unnecessary surgery or otherwise given improper therapy. It also states that 16% of the people in the study made their own diagnosis. I thought this would be good information for the article but I can't find a nice spot to put it. Hopefully someone in the future can integrate this. Triddle 19:23, 15 Apr 2005 (UTC)
- Could you search Pubmed for the relevant reference? That makes inclusion much easier. JFW | T@lk 09:54, 17 Apr 2005 (UTC)
- I can't find a reference to that article on pubmed but pubmed does reference the International Headache Society diagnostic criteria for cluster headache. The report is given to us by the World Headache Alliance which is linked to by IHS with the following qualification: Headache sufferers and their families, or any non-medical person with an interest in this topic, can find information more relevant to their needs at the World Headache Alliance website. That's the strongest reference I can find with my limited medical knowledge. Triddle 22:54, 17 Apr 2005 (UTC)
Link Dispute
Why delete the link to the Cluster Headache Book at med-owl? According to the admin who has twice deleted this link, "let's not advertise other wikis unless very notable in the CH patient community (quod non))." Some thoughts: 1) the fact that another website is a wiki should be irrelevant - would it be better if I put the same information into plain html instead? 2) the page in question is in fact a unique and valuable source of information for the cluster headache community.
Floridian | Talk -- 13:27, July 6, 2005 (signed for the original poster by Wulf January 06)
Here's a quote from the "Cluster Headache Book": "One supplier that has been recommended by several people in the kudzu thread is Vitacost.com Their prices are excellent and they ship to over 50 countries. " The site appears to be nothing more than an "informational storefront" for a vitacost affiliate. Floridian is always on top of the current research on CH but the online book with plugs for vitamin shops worked into the text is inappropriate. The advertising and editorial content must be kept separate. I don't want to get into a revert war, so I'll leave it until Floridian can respond. THB 17:52, 24 February 2006 (UTC)
Wikipedia stated policy is to avoid "Links to sites that primarily exist to sell products or services" and Links to sites with objectionable amounts of advertising. ( http://en.wikipedia.org/wiki/Wikipedia:External_links#Links_normally_to_be_avoided) The CH Book does not primarily exist to sell products or services. The term 'objectionable amount of advertising' is subjective, but comparable with other sites that have not been de-listed. In the case cited above, there have been many people in countries where kudzu is not easily available that have asked about that product, and the fact that a company will ship internationally is a practical issue for patients considering that treatement option.It is one of the largest collections of information on CH written by a patient. Floridian -- Dec 2006)
Featured article
This article should be honed to a standard that would allow it to be the featured article on the front page of Wikipedia so that thousands of people will read it. It will need some illustrations.
Additional fact
A patient of Dr. Robert Nett, a headache specialist, reports that Dr. Nett has said that although CH's are not a commonly occuring condition, is still ranked as the 5th leading cause of suicide among adult males. Those sufferers are usually ones for whom the condition became chronic, without the periods of complete remissinon between clusters of attacks.
I could not find any stats about suicide causes in adult males to verify this.
- —Preceding unsigned comment added by 65.174.156.30 ( talk • contribs) 16:42, 30 March 2006
- A search of PubMed for "cluster headache suicide" gives 5 hits. One of which reviewed world literature on prevalance rates ( PMID 16856701). PMID 737393 makes interesting reading re treatment of patients who have suicidal ideation. PMID 16492244 has potentially relevant title of "Cluster: a potentially lethal headache disorder." but no abstract listed by PubMed (online version requires subscription). David Ruben Talk 01:22, 22 September 2006 (UTC)
A simple web search for "suicide headache" will provide the stats you are seeking. —Preceding unsigned comment added by 98.113.130.91 ( talk) 02:08, 2 March 2010 (UTC)
Other names for cluster headache
According to Silberstein, Lipton, and Goadsby, Horton's Headache actually is an older term for cluster headache.
Older Terms for Cluster Headache
- Erythroprosopalgia of Bing
- Ciliary neuralgia
- Migrainous neuralgia
- Erythromelagia of the head
- Horton's headache
- Histaminic cephalalgia
- Petrosal neuralgia ore spenopalatine neuralgia
- Vidian neuralgia
- Sluder's neuralgia
- Hemicrania angioparalyticia
Stephen D. Silberstein, Richard B. Lipton. Peter J. Goadsby. "Headache in Clinical Practice." Second edition. Taylor & Francis. 2002.
I believe that Sluders Neuralgia is a separate condition and not a different name for cluster headaches. This is alluded to (confusingly) where the article discusses treating them both effectively with lidocaine.
Also, the part about "septoplasty and splinting" is laughable and should be removed as these treatments are not effective for Clusters. The citation (number 10 doesn't even relate to cluster headaches and should also be removed IMHO) The fact that clusters "may" be helped with the administration of lidocaine, in no way indicates that septoplasty and splinting would have ANY effect. The lidocaine numbs the ganglion nerve bundle in the back of the sinus cavity.
Psiloscribe 05:07, 27 June 2007 (UTC)
Since treatment for Sluder's stops a 15-year diagnosis (by several specialists)of Cluster, then what should we call it? Overweight(closes off the nasal passages) adult males (more prone to nose injury via breech birth, etc) experience "adhesions" between 2 or more nasal turbinates - this causes a short circuit of nerve endings that "backfeed" each other, causing intense unilateral "head" pain. Timing of attacks can be altered by smoking, exercise, temperature changes, alcohol, etc. - anything that can swell the membranes can temporarily intensify the pain. Pain killers (lidocaine, etc.)indicate a "pain signal" malfunction. Simple septoplasty and a tiny, temporary splint can separate the turbinates 'till the separated adhesions heal and the pain stops - for good!....This procedure has been used for years - it works. Any good, experienced ENT can confirm this. In short, Sluder's and Cluster are just 2 names for the same rose.
valde 13:21, 30 October 2007
Remove the Illustration
The following discussion is closed. Please do not modify it. Subsequent comments should be made on the appropriate discussion page. No further edits should be made to this discussion.
I propose to remove that creepy illustration/ —The preceding unsigned comment was added by Hawaiianchief ( talk • contribs) 08:25, 10 December 2006 (UTC).
- KEEP - I agree in full that this illustration should stay. When i am personally explaining the pain of a cluster headache i will refer to this site specifically for this illustration. For those of you who object to this, your argument being its graphic nature is not encyclopedic, I would say that an encyclopedia is meant and intended for the education of others. This picture does just that and thus is very encyclopedic. `Cluster Head Dan`
- That is an unbelievably awesome illustration. Please don't remove it. Ever. - Toptomcat 01:56, 6 October 2006 (UTC)
- It is an amazing illustration, but I would happily sign a petition to move it elsewhere on the page - not the main graphic. 82.40.75.55 12:34, 11 December 2006 (UTC)
- Keep - The illustration depicts an artist interpretation of a cluster headache, it's a image most of us sufferer recognise and can relate to. — Preceding unsigned comment added by 109.228.174.129 ( talk) 14:49, 4 October 2012 (UTC)
- Keep - the illustration is fine and in its current location. It is no more creepy than anatomical pictures and gives a clear indication of the type & severity of the problem; indeed I suspect most sufferers would rate the picture as a somewhat gentile underplay of the real severity of an attack. Its location is I feel also appropriate for the same reasons - i.e. in forms an opening backdrop for the discussion that follows. David Ruben Talk 12:56, 11 December 2006 (UTC)
- Keep - the illustration "beautify" encapsulates what I feel when I get one. Jdanb 01:16, 25 January 2007 (UTC)
- Keep absolutely, unless someone has something better with which to replace it. Cluster headaches are creepy. t h b 01:19, 25 January 2007 (UTC)
- STRONG KEEP. Typically I would agree that it should be deleted. But, consider this (and anyone suffering from CH please chime in). When trying to help others understand various conditions people try to give anaolgies or such. For my asthma I tell non-asthmatics to close their nose and breath for 5 minutes through a normal drinking straw. That helps. This illustration is far better than the cliche "ice-pick in the temple". I saw that illustration and cringed because it made the pain's severity and horrid nature very easily understandable to my co-workers (they are CH-free). It is not strictly encyclopedic on the surface...but it is in the spirit of encyclopedic because that picture can let the non-CH sufferer visualize them. All it needs now is that guy jabbing a spike through the eye--but that may be too over-the-top. -- Tony 19:15, 28 March 2007 (UTC)
- VERY strong keep. Despite being a lifelong sufferer of severe headaches, I could only laugh when I saw the image. It perfectly represents the pain that I have felt. PiccoloNamek 12:43, 12 April 2007 (UTC)
- VERY strong keep. I agree with everyone who said to keep it, however, I can see it being a potential problem with various people of different religions. Maybe that "devil" creature can be replaced by some other 'object' stabbing the eye, although I personally do not care because we all know that the devil is a bad thing. It just makes it very clear that cluster headaches are BAD. But like I said, if there's another picture that replaces the devil creature with some other object or something similar, then that would probably be better to use, just for neutrality's sake (if there's such a word). —Preceding unsigned comment added by 64.180.85.99 ( talk • contribs) 08:21, 24 April 2007
- REMOVE. Who cares how evocative it is? You wouldn't find this illustration in a printed encyclopedia, so it doesn't belong here. Goophus 05:09, 11 May 2007 (UTC)
- But Wikipedia is not a print encyclopedia. Wikipedia is not paper. Besides, there is precident for this sort of thing. The images on the sleep paralysis page are a good example.
PiccoloNamek
06:15, 11 May 2007 (UTC)
- Wikipedia certainly hopes to emulate print encyclopedias; otherwise much of the mission statement makes no sense. I agree that artists' interpretations of disorders like this can have a place on a page, but they look bad at the top (particularly in this instance IMO.) And I did not know about the image on this page till a friend (who suffers cluster headaches) made fun of the picture to me, which suggests I'm not the only one who thinks it looks cheesy.
- I don't think a drawing inspired by a King Crimson album cover (to say nothing of the misplaced religious iconography) encourages much trust in the general internet public. Instead it makes wikipedia look horribly amateurish (again IMO.)
Goophus
09:13, 11 May 2007 (UTC)
- You should read
WP:PAPER.
PiccoloNamek
13:31, 11 May 2007 (UTC)
- You should too, because your citation is obnoxious and utterly irrelevant. The gist is contained in the second sentence: ::::"This means that there is no practical limit to the number of topics we can cover, or the total amount of content, other than verifiability and the other points presented on this page." This doesn't mean Wikipedia wants fan-art at the top of its pages, nor does it mean Wikipedia eschews the influence of paper encyclopedias. If it did, perhaps it would be called WikiCarta?
- And certainly nothing is there in your citation to indicate that 'evocative' pics--- which in fact is the only ground on which this piece has been preferred in the above discussion-- should be privileged over descriptive pics, which indeed are already in the body of the article. Why should a wiki article prefer an interpretive image of pain over a far more objective one?
- If you still prefer the page has a cheesy image at the top, that's your business. I'm bowing out of this conversation Goophus 11:27, 15 May 2007 (UTC)
- You should read
WP:PAPER.
PiccoloNamek
13:31, 11 May 2007 (UTC)
- I don't think a drawing inspired by a King Crimson album cover (to say nothing of the misplaced religious iconography) encourages much trust in the general internet public. Instead it makes wikipedia look horribly amateurish (again IMO.)
Goophus
09:13, 11 May 2007 (UTC)
- KEEP, for the reasons given above, or to restate; it perfectly illustrates a condition that has no outwardly visible indicators. Pjbflynn 06:01, 30 July 2007 (UTC)
- Definitely Keep, I have suffered from Cluster Headaches for over 20 years, and that drawing pretty much sums it up. I have used it to show to colleagues and managers, so they can better understand what I'm going through during a bout. —Preceding unsigned comment added by 76.200.158.56 ( talk) 07:19, 27 October 2007 (UTC)
- KEEP, excellent illustration for this entry. A great illustration is a thousand times better than stock photography. DCSB2005 ( talk) 23:13, 1 October 2009 (UTC)
- REMOVING. The image is useful for some people who suffer with CH, but that's irrelevant to the question of the use of the image. Wikipedia is an encyclopedia (First Pillar). I'm boldly removing this image...please reinstate it if you feel the need to. Slowmind ( talk) 17:21, 29 March 2010 (UTC)
- 'KEEP. I am a female sufferer -- I have sent many people (friends, coworkers) to this page, to THIS graphic to try to get across how painful clusters are. It's a wonderful illustration that helps get the point across. Please keep as the primary graphic. 24.107.17.243 ( talk) 19:40, 16 April 2011 (UTC)
- MOVE or REMOVE. While the picture is a fairly accurate graphical representation of a cluster headache I would advocate removing it for one reason alone: the little character on the top has horns suggesting a devil. As I also suffer from cluster headaches I understand the value of the horns on the character, but I wonder if the graphic is not blurring the line between science and religion. The graphic infers that cluster headaches can be remedied by exorcism. The Wikipedia for ‘physician’ does not feature leaches as the main graphic. While I think most people know these remedies are ineffective for most maladies, it may reinforce the notion that refusing medical intervention is a viable option. — Preceding unsigned comment added by Atlrailfan ( talk • contribs) 21:25, 11 January 2012 (UTC)
Currently in the news
Check out that BBC article [1]. Hugo Dufort 06:59, 24 November 2006 (UTC)
Imaging/Pictures
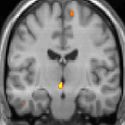
If somebody wants to use them for this article, I put some images into Wikimedia Commons today:
- PET: Activated brain areas during pain
-

-
-




- Voxel based morphometry (VBM, structural)
-

-

-




Click on images and see image description for more information.
-- Friedrich K. 23:29, 23 March 2007 (UTC) (talk)
Done. -- Friedrich K. 08:38, 26 March 2007 (UTC)
Degree of Pain
Hi, one of the sections describes the headaches as "the most severe pain condition known to man." Is there any source for this? It seems as though it is grossely exagerated. Thanks alot. —Preceding unsigned comment added by 99.232.131.105 ( talk • contribs) December 1, 2007
- Quote: "Cluster headache (CH) is one of a group of primary headache disorders (trigeminal autonomic cephalalgias) of uncertain mechanism that are characterized by frequently recurring, short-lasting but extremely severe headache. " Source: http://www.who.int/mediacentre/factsheets/fs277/en/index.html -- Friedrich K. ( talk) 12:19, 25 April 2008 (UTC)
- Peter Goadsby: "Cluster headache is probably the worst pain that humans experience. I know that's quite a strong remark to make, but if you ask a cluster headache patient if they've had a worse experience, they'll universally say they haven't." Source: http://www.abc.net.au/rn/talks/8.30/helthrpt/stories/s42434.htm -- Friedrich K. ( talk) 12:32, 25 April 2008 (UTC)
- So the above 1st ref accepts as "extremely severe headache" and second ref has an important qualifier of "probably the worst pain that humans experience". Therefore neither confirm wording of "the most severe pain condition known to man." - anyway is this wording actually used in the article at the current time ? Second ref is poor source for such a claim, as I'm sure if one asks most cluster headache patients they wont individually have experienced the "hit by a hammer" sudden severity of a sub-arachnoid haemorrhage or the tearing ripping pain of an abdominal aortic aneurism. However clearly we can be reasonable confident that the 1st ref supports comparison to the commonly experenced pains (broken bones, tooth ache, child birth), but for "the worse", one would need a reliable source that systematically compared the pain in CH to all other severe causes of pain. David Ruben Talk 18:06, 25 April 2008 (UTC)
There is no real way of indicating the "worst pain you can ever feel". What hurts me the most may not be the most painful thing to you. —Preceding unsigned comment added by Judd515 ( talk • contribs) 21:42, 27 May 2008 (UTC)
I am one of those rare females who had classic episodic CHs for 22 years before they finally stopped. Typical seasons were two months, twice a year, in spring and fall, with attacks occurring up to five/six times a day, lasting from 15 minutes to three hours. I also had two children during that time, naturally born, without drugs. The first was 8 lbs 8 oz. and a 36 hour labor (a day and a half) with *no pre-softening of the cervix*. The pain involved in that birth was so intense that my brain checked out during transition and I thought for a moment that I was somewhere else. The second child took only 3 hours to bear, and was 10 lbs 10 oz. Also pretty intense. But in no way would the pain of either of these births hold a candle to the typical cluster headache I experienced.
I believe that this is because most kinds of pain benefit from the release of endorphins (and whatever other opiate-like drugs our bodies typically release when we are in pain), but cluster headaches are made *worse* by these drugs. In fact, while I was in the hospital after my first baby was born, I went into an uncharacteristic CH season, getting attacks right there in the hospital. I was given morphine for the pain of the aftermath of childbirth, and when I took it, the morphine actually made the cluster headache I was having much more intense. I refused all pain killers after that, because I knew they would make the clusters worse.
The point being, the intensity of the pain of cluster headaches is made more unbearable by the very mechanism of the headache: that it grows in intensity in response to the very drugs our bodies use to shield us from pain. You might not want to stick your hand over a steaming kettle for a half hour, but I guarantee that if you did, your endorphins and whatnot would kick in and help you tremendously for at least the last 25 minutes of that experience (in fact, you would probably pass out). Not so with cluster headaches. The intensity of the pain is that brand of intensity that we might also experience in having our eyelids held open and being forced to watch while some horrid event unfolded before us. I can't tell you how many times I jumped out of bed and ran around the room, or sometimes even the neighborhood, flailing my arms and trying to wake my body up before an oncoming attack took hold when I was a teenager/young adult, because I knew that as bad as it might be when awake, if I got caught while sleeping (or even relaxing) it was going to be many times worse. There is something very chemically different about this kind of pain--something that truly makes it incomparable to other types of pain. I hesitate now to even tell sufferers who are only a few years into it that mine lasted 22 years.
69.109.122.108 ( talk) 06:02, 19 December 2009 (UTC)Leha Carpenter
History
PMC 1813127 goes greatly into the history of the disease and its nomenclature. Descriptions from 1908 and 1926 predate Horton's paper. JFW | T@lk 20:43, 27 May 2008 (UTC)
- The first complete description of cluster headache was given by the London neurologist Wilfred Harris in 1926. Added this to the article today. Early case reports have been found from Nicolaes Tulp - 1641 and from Gerard van Swieten - 1745. Please see http://ck-wissen.de/ckwiki/index.php?title=Geschichte_des_Cluster-Kopfschmerzes (German) for refs and more details on cluster headache history. -- Friedrich K. ( talk) 20:48, 13 August 2008 (UTC)
IHS Classification ICHD-II
Episodic cluster headache G44.01
Chronic cluster headache G44.02
Zouhair ( talk) 17:34, 6 August 2009 (UTC)
High flow O2 works double blind
Goadsby and his people at Queen's Square have done an RCT with oxygen: http://jama.ama-assn.org/cgi/content/abstract/302/22/2451 JFW | T@lk 22:32, 8 December 2009 (UTC)
Why no discussion of Histamine Desensitization ?
I was wondering why there isn't any mention of Histamine Desensitization therapy for the treatment of Cluster Headaches ? I don't feel that it will work for every cluster patient, but I KNOW it will work for some, as I have myself have reaped great success from the treatment. I also met others with Cluster Headaches which flew from great distances to Chicago's Diamond Headache Clinic to have this treatment with great success.
The treatment failed for me a couple of times in a row at first, and then, it worked at stopping all of my attacks for approximately 9 weeks, then the process had to be repeated. I went through this for a few years before the attacks stopped (after taking a drug called "Savella", which may be just a coincidence, or may have stopped my chronic clusters).
There are articles out there to support the claim the Histamine will help some sufferers and plenty of patients to support that claim, with the proper research. Dr. Seymour Diamond or his daughter, Merle Diamond, from the Diamond Headache Clinic can provide clinical result trial statistics, and other information that you may wish to know.
To sum this letter up, I just ask that you include Histamine Desensitization Therapy as a treatment option that may help some Cluster Headache patients. this is not intended to "slam" any other treatments, although there are some that I find ridiculous. Please consider adding Histamine Desensitization Therapy as an option. It may help many people and change their lives for the better. Who knows, it could even save some lives !!
Thank You for your time in reading this and I hope you seriously consider my question.
A 21 year Cluster Headache sufferer. (13 years episodic & 8 more years Chronic)...I'm now cluster free for just over 100 days and I feel like I have a new leash on life !!
Respectfully,
09:28, 25 January 2010 (UTC) SOLVED 09:28, 25 January 2010 (UTC)
- QUOTE: "Intractable cluster headaches have been successfully treated with intravenous histamine desensitization." FROM: http://diamondheadache.com/article_archives/cluster_headache.html
- QUOTE IN PARTIAL:"Although it has been asserted that histamine desensitization therapy is of benefit patients with intractable migraine and cluster headaches (see, e.g., Freitag, 2004; Biondi & Mendes, 2004)" FROM: http://www.aetna.com/cpb/medical/data/600_699/0647.html
- QUOTE:"One of the earliest descriptions of the different forms of cluster headaches (episodic vs. chronic) was given by Bayard T. Horton, M.D. (1895-1980), of Mayo Clinic. Doctor Horton treated many of his chronic cluster headache patients with intravenous histamine desensitization." FROM:(A BOOK)"Cluster Headaches:Treatment and Relief for Cluster, Cluster Migraine, And Recurring Eye-Stab Pain"; See URL: http://thinktwice.com/clusters.htm
Thanks !! —Preceding unsigned comment added by 74.142.185.27 ( talk) 09:28, 25 January 2010 (UTC)
Triggers
From the "Triggers" section, "Ingestion of alcohol or chocolate or banana are recognized as a common trigger". Alcohol, fine, nearly everyone agrees that alcohol is guaranteed to cause an attack. The others I've never heard of being common CH triggers, especially banana. Maybe they triggered a hit in someone, but they're not common. At any rate, it's uncited. Next, "Lahore or 'chinese salt' is nearly always a triger of migraines. Sexual frustration, Sex or Orgasms may trigger Cluster Headaches in some patients." First, we're not talking about migranes. And again, I can't find any external mention of any of these related to triggering CH attacks. Sexual frustration?? Seriously?
Really, nearly this entire section is anecdotal. I think the article would be better served mentioning Nitroglycerin (I believe subcutaneously), alcohol (since it is the most common and widely reported trigger), and beyond that just that vasodilators generally can be expected to trigger an attack when in cycle. Maybe keep the part "The role of diet and specific foods in triggering cluster headaches is controversial and not well understood." Right now, it sounds like a bunch of edits from people that got headaches after eating sushi, so they added "and sushi too!" Greghodg ( talk) 17:49, 4 August 2010 (UTC)
Deep brain stimulation
Why is there no mention of deep brain stimulation on this page? Take a look at this link: http://www.bbc.co.uk/blogs/thereporters/ferguswalsh/2010/12/brain_surgery_to_relieve_headaches.html Reissgo ( talk) 08:34, 18 December 2010 (UTC)
LSD
===Low-dose psychedelics===
There is anecdotal evidence that serotonergic psychedelics such as psilocybin (mushrooms), LSD, and LSA ( d-Lysergic acid amide, contained by Rivea corymbosa seeds) abort cluster periods and extend remission periods. The doses needed to affect cluster headaches start below those needed to produce psychedelic effects. [1] [2] [3] Melatonin, psilocybin, serotonin, and the triptan abortive drugs are closely-related tryptamines.
Researchers at McLean Hospital/Harvard Medical School investigated the ability of psilocybin ("magic mushrooms") and LSD to treat cluster headaches through medical record review and interview of 53 patients who had used either/both drug, reporting in Neurology that the majority described partial or complete relief from cluster attacks. [4] A clinical study of these treatments under the auspices of Clusterbusters is the next intended phase of research at McLean Hospital, Harvard Medical School. [5] [6]
This needs to be based on review articles per WP:MEDRS Doc James ( talk · contribs · email) 13:21, 19 January 2011 (UTC)
- Here's one: Sun-Edelstein C, Mauskop A. (2011). "Alternative headache treatments: nutraceuticals, behavioral and physical treatments". Headache: the Journal of Head and Face Pain. 51 (3): 469–83. doi: 10.1111/j.1526-4610.2011.01846.x. PMID 21352222. Sasata ( talk) 05:22, 17 November 2011 (UTC)
Infobox image
At the moment, Clusterhead.jpg is the image in the infobox, visible at the very top of the page. While this image may be useful later in the article, I am of the opinion that as far as lead images go, this is actually worse than having no image at all. Quickly jumping from the article title to this image will lead the reader to believe that the article is about a piece of art, and certainly not a medical condition. I welcome arguments or suggestions, but if no one objects, I may just swap out the image myself. -- Cryptic C62 · Talk 04:39, 17 November 2011 (UTC)
{kind=link}
- It's now been removed. — Hex (❝?!❞) 11:55, 5 November 2012 (UTC)
"Atypical Facial Pain Syndrome"
This comment has been hidden, as
Wikipedia does not provide medical advice.
|
|---|
| Wikipedia does not provide medical advice. The following comment seeks medical advice. This is not a suitable place. Please seek a real-life medical professional. Comments from well-meaning Wikipedians may not represent best practice in the poster's country of origin, and there is a danger that best practice may be misrepresented or, at worst, deliberately distorted. No further edits should be made to this discussion. |
|
I was sent to an ONT who said I had "Atypical Facial Pain Syndrome". When I said "that doesn't really say anything other than what I just described to you" he said "it's also known as cluster migraines." Is this generally accepted? I ask because I see no reference to it here. -- Richardson mcphillips ( talk) 19:48, 14 March 2012 (UTC)
|
2012 review in the BMJ
[2] Doc James ( talk · contribs · email) 08:15, 15 April 2012 (UTC)
Copyright
Copyright violating content is illegal and cannot be allowed in the articles. However, the following citation may be useful:
causa sui ( talk) 18:33, 19 May 2013 (UTC)
- A) The text you removed was the following sentence:
- Although controversial, case reports suggest that ingesting psilocybin or LSD can reduce cluster headache pain and interrupt cluster headache cycles.
- The abstract, located
here, contains the following sentence:
- Although controversial, there are some reports demonstrating the benefit of recreational drugs such as marijuana, lysergic acid diethylamide and psilocybin in headache treatment.
- With the exception of the initial two words, "Although controversial", the two sentences are almost completely different. Your robust assertion of a "copyright violation" is baffling, when simply removing those two words would have done. See WP:LIMITED.
- B) You clearly didn't bother to read the diff before blindly hitting revert, as I had fixed the problem while undoing your strange deletion. The text in my version read:
- Some case reports have also suggested that ingesting LSD, psilocybin or cannabis can reduce cluster headache pain and interrupt cluster headache cycles.
- Consequently I have now restored it. — Scott • talk 22:38, 19 May 2013 (UTC)
Psilocybin and LSD
As a casual reader, this section strikes me as odd, for this line: "For many sufferers, the legal risks pale in comparison to the pain caused by the condition.[citation needed]", specifically the need for the citation? As the article has already established several times that people are willing to commit suicide to end the pain, and those are cited. So I feel that there's no need for a source - it's just reasonable to assume that any legal problems would not be as big of a deal to plenty of people who are suicidal. — Preceding unsigned comment added by 50.124.52.204 ( talk) 04:57, 1 June 2013 (UTC)
- The source is necessary because conclusions drawn by the writer are agains WP:NOR PinkShinyRose ( talk) 20:58, 28 July 2013 (UTC)
Bias: introduction of the "Management" section, third paragraph
Except for the first sentence this paragraph is only relevant to the US. I think the first sentence should remain (maybe rephrased to fit into a prior paragraph), but the remaining part of the paragraph should be separate and start out by explicitly stating that it is relevant only to the US (maybe by starting the paragraph by "In the US there are difficulties in treatment arising from the recent pressure of the DEA. Depending on the state...". Should the first sentence be rephrased or just appended to the previous paragraph? Does anyone disagree about clarifying the limited scope of the paragraph in the first sentence? PinkShinyRose ( talk) 21:08, 28 July 2013 (UTC)
merger proposal: Cluster headache treatments
I don't see anything especially notable in the other page that isnt already here, and I don't see the point of this redundancy. It also tends to be a spam/NPOV attractor. -- [ UseTheCommandLine ~/ talk ]# ▄ 17:59, 28 August 2013 (UTC)
- I didn't know that existed. It should definitely be merged here. — Scott • talk 22:09, 28 August 2013 (UTC)
I have completed the merge. This page needs additional attention and I would be happy to collaboratively edit if there are any interested editors. LT90001 ( talk) 03:05, 12 October 2013 (UTC)
Cleanup
- Edit: I refer to this edit, removing my cleanup tags.
I have marked this page for cleanup because it uses numerous primary sources, has excessive use of dated, experimental or primary sources, with conflicting advice; and requires general copy-editing. This is not a comment on a particular source or treatment methodology, just that this article needs some work overall. Kind regards, LT910001 ( talk) 04:18, 13 October 2013 (UTC)
| This is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 |
- ^ "Hallucinogenic Treatment of Neuro-Vascular Headaches". ClusterBusters. Retrieved 2006-09-22.
- ^ Mark Honigsbaum (2005-08-02). "Headache sufferers flout new drug law - Calls for clinical trials and rethink of legislation as patients claim that magic mushrooms can relieve excruciating condition". The Guardian. Retrieved 2006-09-22. [reprint by Multidisciplinary Association for Psychedelic Studies]
- ^ Arran Frood (2008-10-07). "LSD cured my headache - Cluster headaches cause such severe pain that some sufferers are driven to suicide. Now one man believes he's found a surprising cure". The Independent. Retrieved 2008-10-07.
-
^ Sewell R, Halpern J, Pope H (2006).
"Response of cluster headache to psilocybin and LSD" (
PDF). Neurology. 66 (12): 1920–2.
doi:
10.1212/01.wnl.0000219761.05466.43.
PMID
16801660.
{{ cite journal}}: Unknown parameter|month=ignored ( help)CS1 maint: multiple names: authors list ( link) - a Brief Communications, also presented as:
Sewell, R. Andrew, M.D.; Halpern, John M., M.D. "The Effects Of Psilocybin And LSD On Cluster Headache: A Series Of 53 Cases." Abstract. Presented to the National Headache Foundation’s Annual Headache Research Summit. February, 2006. Twenty-two of 26 psilocybin users reported that psilocybin aborted attacks; 25 of 48 psilocybin users and 7 of 8 LSD users reported cluster period termination; 18 of 19 psilocybin users and 4 of 5 LSD users reported remission period extension. - ^ "Research into psilocybin and LSD as potential treatments for people with cluster headaches". LSD and Psilocybin Research. Multidisciplinary Association for Psychedelic Studies. Retrieved 2006-09-22.
- ^ "Response of Cluster Headache to Psilocybin and LSD" Chapter 5 in "Psychedelic Medicine: New Evidence for Hallucinogens as Treatment" Michael Winkelman and Thomas B. Roberts (editors) (2007) Westport, CT: Praeger/Greenwood.
| This is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 |
Misdiagnosis Article at WHA
I was researching cluster headaches and I found Vast Majority of Cluster Headache Patients Are Initially Misdiagnosed. In short it says that most doctors were unable to properly identify cluster headache in the majority of patients. Some were led to unnecessary surgery or otherwise given improper therapy. It also states that 16% of the people in the study made their own diagnosis. I thought this would be good information for the article but I can't find a nice spot to put it. Hopefully someone in the future can integrate this. Triddle 19:23, 15 Apr 2005 (UTC)
- Could you search Pubmed for the relevant reference? That makes inclusion much easier. JFW | T@lk 09:54, 17 Apr 2005 (UTC)
- I can't find a reference to that article on pubmed but pubmed does reference the International Headache Society diagnostic criteria for cluster headache. The report is given to us by the World Headache Alliance which is linked to by IHS with the following qualification: Headache sufferers and their families, or any non-medical person with an interest in this topic, can find information more relevant to their needs at the World Headache Alliance website. That's the strongest reference I can find with my limited medical knowledge. Triddle 22:54, 17 Apr 2005 (UTC)
Link Dispute
Why delete the link to the Cluster Headache Book at med-owl? According to the admin who has twice deleted this link, "let's not advertise other wikis unless very notable in the CH patient community (quod non))." Some thoughts: 1) the fact that another website is a wiki should be irrelevant - would it be better if I put the same information into plain html instead? 2) the page in question is in fact a unique and valuable source of information for the cluster headache community.
Floridian | Talk -- 13:27, July 6, 2005 (signed for the original poster by Wulf January 06)
Here's a quote from the "Cluster Headache Book": "One supplier that has been recommended by several people in the kudzu thread is Vitacost.com Their prices are excellent and they ship to over 50 countries. " The site appears to be nothing more than an "informational storefront" for a vitacost affiliate. Floridian is always on top of the current research on CH but the online book with plugs for vitamin shops worked into the text is inappropriate. The advertising and editorial content must be kept separate. I don't want to get into a revert war, so I'll leave it until Floridian can respond. THB 17:52, 24 February 2006 (UTC)
Wikipedia stated policy is to avoid "Links to sites that primarily exist to sell products or services" and Links to sites with objectionable amounts of advertising. ( http://en.wikipedia.org/wiki/Wikipedia:External_links#Links_normally_to_be_avoided) The CH Book does not primarily exist to sell products or services. The term 'objectionable amount of advertising' is subjective, but comparable with other sites that have not been de-listed. In the case cited above, there have been many people in countries where kudzu is not easily available that have asked about that product, and the fact that a company will ship internationally is a practical issue for patients considering that treatement option.It is one of the largest collections of information on CH written by a patient. Floridian -- Dec 2006)
Featured article
This article should be honed to a standard that would allow it to be the featured article on the front page of Wikipedia so that thousands of people will read it. It will need some illustrations.
Additional fact
A patient of Dr. Robert Nett, a headache specialist, reports that Dr. Nett has said that although CH's are not a commonly occuring condition, is still ranked as the 5th leading cause of suicide among adult males. Those sufferers are usually ones for whom the condition became chronic, without the periods of complete remissinon between clusters of attacks.
I could not find any stats about suicide causes in adult males to verify this.
- —Preceding unsigned comment added by 65.174.156.30 ( talk • contribs) 16:42, 30 March 2006
- A search of PubMed for "cluster headache suicide" gives 5 hits. One of which reviewed world literature on prevalance rates ( PMID 16856701). PMID 737393 makes interesting reading re treatment of patients who have suicidal ideation. PMID 16492244 has potentially relevant title of "Cluster: a potentially lethal headache disorder." but no abstract listed by PubMed (online version requires subscription). David Ruben Talk 01:22, 22 September 2006 (UTC)
A simple web search for "suicide headache" will provide the stats you are seeking. —Preceding unsigned comment added by 98.113.130.91 ( talk) 02:08, 2 March 2010 (UTC)
Other names for cluster headache
According to Silberstein, Lipton, and Goadsby, Horton's Headache actually is an older term for cluster headache.
Older Terms for Cluster Headache
- Erythroprosopalgia of Bing
- Ciliary neuralgia
- Migrainous neuralgia
- Erythromelagia of the head
- Horton's headache
- Histaminic cephalalgia
- Petrosal neuralgia ore spenopalatine neuralgia
- Vidian neuralgia
- Sluder's neuralgia
- Hemicrania angioparalyticia
Stephen D. Silberstein, Richard B. Lipton. Peter J. Goadsby. "Headache in Clinical Practice." Second edition. Taylor & Francis. 2002.
I believe that Sluders Neuralgia is a separate condition and not a different name for cluster headaches. This is alluded to (confusingly) where the article discusses treating them both effectively with lidocaine.
Also, the part about "septoplasty and splinting" is laughable and should be removed as these treatments are not effective for Clusters. The citation (number 10 doesn't even relate to cluster headaches and should also be removed IMHO) The fact that clusters "may" be helped with the administration of lidocaine, in no way indicates that septoplasty and splinting would have ANY effect. The lidocaine numbs the ganglion nerve bundle in the back of the sinus cavity.
Psiloscribe 05:07, 27 June 2007 (UTC)
Since treatment for Sluder's stops a 15-year diagnosis (by several specialists)of Cluster, then what should we call it? Overweight(closes off the nasal passages) adult males (more prone to nose injury via breech birth, etc) experience "adhesions" between 2 or more nasal turbinates - this causes a short circuit of nerve endings that "backfeed" each other, causing intense unilateral "head" pain. Timing of attacks can be altered by smoking, exercise, temperature changes, alcohol, etc. - anything that can swell the membranes can temporarily intensify the pain. Pain killers (lidocaine, etc.)indicate a "pain signal" malfunction. Simple septoplasty and a tiny, temporary splint can separate the turbinates 'till the separated adhesions heal and the pain stops - for good!....This procedure has been used for years - it works. Any good, experienced ENT can confirm this. In short, Sluder's and Cluster are just 2 names for the same rose.
valde 13:21, 30 October 2007
Remove the Illustration
The following discussion is closed. Please do not modify it. Subsequent comments should be made on the appropriate discussion page. No further edits should be made to this discussion.
I propose to remove that creepy illustration/ —The preceding unsigned comment was added by Hawaiianchief ( talk • contribs) 08:25, 10 December 2006 (UTC).
- KEEP - I agree in full that this illustration should stay. When i am personally explaining the pain of a cluster headache i will refer to this site specifically for this illustration. For those of you who object to this, your argument being its graphic nature is not encyclopedic, I would say that an encyclopedia is meant and intended for the education of others. This picture does just that and thus is very encyclopedic. `Cluster Head Dan`
- That is an unbelievably awesome illustration. Please don't remove it. Ever. - Toptomcat 01:56, 6 October 2006 (UTC)
- It is an amazing illustration, but I would happily sign a petition to move it elsewhere on the page - not the main graphic. 82.40.75.55 12:34, 11 December 2006 (UTC)
- Keep - The illustration depicts an artist interpretation of a cluster headache, it's a image most of us sufferer recognise and can relate to. — Preceding unsigned comment added by 109.228.174.129 ( talk) 14:49, 4 October 2012 (UTC)
- Keep - the illustration is fine and in its current location. It is no more creepy than anatomical pictures and gives a clear indication of the type & severity of the problem; indeed I suspect most sufferers would rate the picture as a somewhat gentile underplay of the real severity of an attack. Its location is I feel also appropriate for the same reasons - i.e. in forms an opening backdrop for the discussion that follows. David Ruben Talk 12:56, 11 December 2006 (UTC)
- Keep - the illustration "beautify" encapsulates what I feel when I get one. Jdanb 01:16, 25 January 2007 (UTC)
- Keep absolutely, unless someone has something better with which to replace it. Cluster headaches are creepy. t h b 01:19, 25 January 2007 (UTC)
- STRONG KEEP. Typically I would agree that it should be deleted. But, consider this (and anyone suffering from CH please chime in). When trying to help others understand various conditions people try to give anaolgies or such. For my asthma I tell non-asthmatics to close their nose and breath for 5 minutes through a normal drinking straw. That helps. This illustration is far better than the cliche "ice-pick in the temple". I saw that illustration and cringed because it made the pain's severity and horrid nature very easily understandable to my co-workers (they are CH-free). It is not strictly encyclopedic on the surface...but it is in the spirit of encyclopedic because that picture can let the non-CH sufferer visualize them. All it needs now is that guy jabbing a spike through the eye--but that may be too over-the-top. -- Tony 19:15, 28 March 2007 (UTC)
- VERY strong keep. Despite being a lifelong sufferer of severe headaches, I could only laugh when I saw the image. It perfectly represents the pain that I have felt. PiccoloNamek 12:43, 12 April 2007 (UTC)
- VERY strong keep. I agree with everyone who said to keep it, however, I can see it being a potential problem with various people of different religions. Maybe that "devil" creature can be replaced by some other 'object' stabbing the eye, although I personally do not care because we all know that the devil is a bad thing. It just makes it very clear that cluster headaches are BAD. But like I said, if there's another picture that replaces the devil creature with some other object or something similar, then that would probably be better to use, just for neutrality's sake (if there's such a word). —Preceding unsigned comment added by 64.180.85.99 ( talk • contribs) 08:21, 24 April 2007
- REMOVE. Who cares how evocative it is? You wouldn't find this illustration in a printed encyclopedia, so it doesn't belong here. Goophus 05:09, 11 May 2007 (UTC)
- But Wikipedia is not a print encyclopedia. Wikipedia is not paper. Besides, there is precident for this sort of thing. The images on the sleep paralysis page are a good example.
PiccoloNamek
06:15, 11 May 2007 (UTC)
- Wikipedia certainly hopes to emulate print encyclopedias; otherwise much of the mission statement makes no sense. I agree that artists' interpretations of disorders like this can have a place on a page, but they look bad at the top (particularly in this instance IMO.) And I did not know about the image on this page till a friend (who suffers cluster headaches) made fun of the picture to me, which suggests I'm not the only one who thinks it looks cheesy.
- I don't think a drawing inspired by a King Crimson album cover (to say nothing of the misplaced religious iconography) encourages much trust in the general internet public. Instead it makes wikipedia look horribly amateurish (again IMO.)
Goophus
09:13, 11 May 2007 (UTC)
- You should read
WP:PAPER.
PiccoloNamek
13:31, 11 May 2007 (UTC)
- You should too, because your citation is obnoxious and utterly irrelevant. The gist is contained in the second sentence: ::::"This means that there is no practical limit to the number of topics we can cover, or the total amount of content, other than verifiability and the other points presented on this page." This doesn't mean Wikipedia wants fan-art at the top of its pages, nor does it mean Wikipedia eschews the influence of paper encyclopedias. If it did, perhaps it would be called WikiCarta?
- And certainly nothing is there in your citation to indicate that 'evocative' pics--- which in fact is the only ground on which this piece has been preferred in the above discussion-- should be privileged over descriptive pics, which indeed are already in the body of the article. Why should a wiki article prefer an interpretive image of pain over a far more objective one?
- If you still prefer the page has a cheesy image at the top, that's your business. I'm bowing out of this conversation Goophus 11:27, 15 May 2007 (UTC)
- You should read
WP:PAPER.
PiccoloNamek
13:31, 11 May 2007 (UTC)
- I don't think a drawing inspired by a King Crimson album cover (to say nothing of the misplaced religious iconography) encourages much trust in the general internet public. Instead it makes wikipedia look horribly amateurish (again IMO.)
Goophus
09:13, 11 May 2007 (UTC)
- KEEP, for the reasons given above, or to restate; it perfectly illustrates a condition that has no outwardly visible indicators. Pjbflynn 06:01, 30 July 2007 (UTC)
- Definitely Keep, I have suffered from Cluster Headaches for over 20 years, and that drawing pretty much sums it up. I have used it to show to colleagues and managers, so they can better understand what I'm going through during a bout. —Preceding unsigned comment added by 76.200.158.56 ( talk) 07:19, 27 October 2007 (UTC)
- KEEP, excellent illustration for this entry. A great illustration is a thousand times better than stock photography. DCSB2005 ( talk) 23:13, 1 October 2009 (UTC)
- REMOVING. The image is useful for some people who suffer with CH, but that's irrelevant to the question of the use of the image. Wikipedia is an encyclopedia (First Pillar). I'm boldly removing this image...please reinstate it if you feel the need to. Slowmind ( talk) 17:21, 29 March 2010 (UTC)
- 'KEEP. I am a female sufferer -- I have sent many people (friends, coworkers) to this page, to THIS graphic to try to get across how painful clusters are. It's a wonderful illustration that helps get the point across. Please keep as the primary graphic. 24.107.17.243 ( talk) 19:40, 16 April 2011 (UTC)
- MOVE or REMOVE. While the picture is a fairly accurate graphical representation of a cluster headache I would advocate removing it for one reason alone: the little character on the top has horns suggesting a devil. As I also suffer from cluster headaches I understand the value of the horns on the character, but I wonder if the graphic is not blurring the line between science and religion. The graphic infers that cluster headaches can be remedied by exorcism. The Wikipedia for ‘physician’ does not feature leaches as the main graphic. While I think most people know these remedies are ineffective for most maladies, it may reinforce the notion that refusing medical intervention is a viable option. — Preceding unsigned comment added by Atlrailfan ( talk • contribs) 21:25, 11 January 2012 (UTC)
Currently in the news
Check out that BBC article [1]. Hugo Dufort 06:59, 24 November 2006 (UTC)
Imaging/Pictures
If somebody wants to use them for this article, I put some images into Wikimedia Commons today:
- PET: Activated brain areas during pain
-
-
-
- Voxel based morphometry (VBM, structural)
-
-
-
Click on images and see image description for more information.
-- Friedrich K. 23:29, 23 March 2007 (UTC) (talk)
Done. -- Friedrich K. 08:38, 26 March 2007 (UTC)
Degree of Pain
Hi, one of the sections describes the headaches as "the most severe pain condition known to man." Is there any source for this? It seems as though it is grossely exagerated. Thanks alot. —Preceding unsigned comment added by 99.232.131.105 ( talk • contribs) December 1, 2007
- Quote: "Cluster headache (CH) is one of a group of primary headache disorders (trigeminal autonomic cephalalgias) of uncertain mechanism that are characterized by frequently recurring, short-lasting but extremely severe headache. " Source: http://www.who.int/mediacentre/factsheets/fs277/en/index.html -- Friedrich K. ( talk) 12:19, 25 April 2008 (UTC)
- Peter Goadsby: "Cluster headache is probably the worst pain that humans experience. I know that's quite a strong remark to make, but if you ask a cluster headache patient if they've had a worse experience, they'll universally say they haven't." Source: http://www.abc.net.au/rn/talks/8.30/helthrpt/stories/s42434.htm -- Friedrich K. ( talk) 12:32, 25 April 2008 (UTC)
- So the above 1st ref accepts as "extremely severe headache" and second ref has an important qualifier of "probably the worst pain that humans experience". Therefore neither confirm wording of "the most severe pain condition known to man." - anyway is this wording actually used in the article at the current time ? Second ref is poor source for such a claim, as I'm sure if one asks most cluster headache patients they wont individually have experienced the "hit by a hammer" sudden severity of a sub-arachnoid haemorrhage or the tearing ripping pain of an abdominal aortic aneurism. However clearly we can be reasonable confident that the 1st ref supports comparison to the commonly experenced pains (broken bones, tooth ache, child birth), but for "the worse", one would need a reliable source that systematically compared the pain in CH to all other severe causes of pain. David Ruben Talk 18:06, 25 April 2008 (UTC)
There is no real way of indicating the "worst pain you can ever feel". What hurts me the most may not be the most painful thing to you. —Preceding unsigned comment added by Judd515 ( talk • contribs) 21:42, 27 May 2008 (UTC)
I am one of those rare females who had classic episodic CHs for 22 years before they finally stopped. Typical seasons were two months, twice a year, in spring and fall, with attacks occurring up to five/six times a day, lasting from 15 minutes to three hours. I also had two children during that time, naturally born, without drugs. The first was 8 lbs 8 oz. and a 36 hour labor (a day and a half) with *no pre-softening of the cervix*. The pain involved in that birth was so intense that my brain checked out during transition and I thought for a moment that I was somewhere else. The second child took only 3 hours to bear, and was 10 lbs 10 oz. Also pretty intense. But in no way would the pain of either of these births hold a candle to the typical cluster headache I experienced.
I believe that this is because most kinds of pain benefit from the release of endorphins (and whatever other opiate-like drugs our bodies typically release when we are in pain), but cluster headaches are made *worse* by these drugs. In fact, while I was in the hospital after my first baby was born, I went into an uncharacteristic CH season, getting attacks right there in the hospital. I was given morphine for the pain of the aftermath of childbirth, and when I took it, the morphine actually made the cluster headache I was having much more intense. I refused all pain killers after that, because I knew they would make the clusters worse.
The point being, the intensity of the pain of cluster headaches is made more unbearable by the very mechanism of the headache: that it grows in intensity in response to the very drugs our bodies use to shield us from pain. You might not want to stick your hand over a steaming kettle for a half hour, but I guarantee that if you did, your endorphins and whatnot would kick in and help you tremendously for at least the last 25 minutes of that experience (in fact, you would probably pass out). Not so with cluster headaches. The intensity of the pain is that brand of intensity that we might also experience in having our eyelids held open and being forced to watch while some horrid event unfolded before us. I can't tell you how many times I jumped out of bed and ran around the room, or sometimes even the neighborhood, flailing my arms and trying to wake my body up before an oncoming attack took hold when I was a teenager/young adult, because I knew that as bad as it might be when awake, if I got caught while sleeping (or even relaxing) it was going to be many times worse. There is something very chemically different about this kind of pain--something that truly makes it incomparable to other types of pain. I hesitate now to even tell sufferers who are only a few years into it that mine lasted 22 years.
69.109.122.108 ( talk) 06:02, 19 December 2009 (UTC)Leha Carpenter
History
PMC 1813127 goes greatly into the history of the disease and its nomenclature. Descriptions from 1908 and 1926 predate Horton's paper. JFW | T@lk 20:43, 27 May 2008 (UTC)
- The first complete description of cluster headache was given by the London neurologist Wilfred Harris in 1926. Added this to the article today. Early case reports have been found from Nicolaes Tulp - 1641 and from Gerard van Swieten - 1745. Please see http://ck-wissen.de/ckwiki/index.php?title=Geschichte_des_Cluster-Kopfschmerzes (German) for refs and more details on cluster headache history. -- Friedrich K. ( talk) 20:48, 13 August 2008 (UTC)
IHS Classification ICHD-II
Episodic cluster headache G44.01
Chronic cluster headache G44.02
Zouhair ( talk) 17:34, 6 August 2009 (UTC)
High flow O2 works double blind
Goadsby and his people at Queen's Square have done an RCT with oxygen: http://jama.ama-assn.org/cgi/content/abstract/302/22/2451 JFW | T@lk 22:32, 8 December 2009 (UTC)
Why no discussion of Histamine Desensitization ?
I was wondering why there isn't any mention of Histamine Desensitization therapy for the treatment of Cluster Headaches ? I don't feel that it will work for every cluster patient, but I KNOW it will work for some, as I have myself have reaped great success from the treatment. I also met others with Cluster Headaches which flew from great distances to Chicago's Diamond Headache Clinic to have this treatment with great success.
The treatment failed for me a couple of times in a row at first, and then, it worked at stopping all of my attacks for approximately 9 weeks, then the process had to be repeated. I went through this for a few years before the attacks stopped (after taking a drug called "Savella", which may be just a coincidence, or may have stopped my chronic clusters).
There are articles out there to support the claim the Histamine will help some sufferers and plenty of patients to support that claim, with the proper research. Dr. Seymour Diamond or his daughter, Merle Diamond, from the Diamond Headache Clinic can provide clinical result trial statistics, and other information that you may wish to know.
To sum this letter up, I just ask that you include Histamine Desensitization Therapy as a treatment option that may help some Cluster Headache patients. this is not intended to "slam" any other treatments, although there are some that I find ridiculous. Please consider adding Histamine Desensitization Therapy as an option. It may help many people and change their lives for the better. Who knows, it could even save some lives !!
Thank You for your time in reading this and I hope you seriously consider my question.
A 21 year Cluster Headache sufferer. (13 years episodic & 8 more years Chronic)...I'm now cluster free for just over 100 days and I feel like I have a new leash on life !!
Respectfully,
09:28, 25 January 2010 (UTC) SOLVED 09:28, 25 January 2010 (UTC)
- QUOTE: "Intractable cluster headaches have been successfully treated with intravenous histamine desensitization." FROM: http://diamondheadache.com/article_archives/cluster_headache.html
- QUOTE IN PARTIAL:"Although it has been asserted that histamine desensitization therapy is of benefit patients with intractable migraine and cluster headaches (see, e.g., Freitag, 2004; Biondi & Mendes, 2004)" FROM: http://www.aetna.com/cpb/medical/data/600_699/0647.html
- QUOTE:"One of the earliest descriptions of the different forms of cluster headaches (episodic vs. chronic) was given by Bayard T. Horton, M.D. (1895-1980), of Mayo Clinic. Doctor Horton treated many of his chronic cluster headache patients with intravenous histamine desensitization." FROM:(A BOOK)"Cluster Headaches:Treatment and Relief for Cluster, Cluster Migraine, And Recurring Eye-Stab Pain"; See URL: http://thinktwice.com/clusters.htm
Thanks !! —Preceding unsigned comment added by 74.142.185.27 ( talk) 09:28, 25 January 2010 (UTC)
Triggers
From the "Triggers" section, "Ingestion of alcohol or chocolate or banana are recognized as a common trigger". Alcohol, fine, nearly everyone agrees that alcohol is guaranteed to cause an attack. The others I've never heard of being common CH triggers, especially banana. Maybe they triggered a hit in someone, but they're not common. At any rate, it's uncited. Next, "Lahore or 'chinese salt' is nearly always a triger of migraines. Sexual frustration, Sex or Orgasms may trigger Cluster Headaches in some patients." First, we're not talking about migranes. And again, I can't find any external mention of any of these related to triggering CH attacks. Sexual frustration?? Seriously?
Really, nearly this entire section is anecdotal. I think the article would be better served mentioning Nitroglycerin (I believe subcutaneously), alcohol (since it is the most common and widely reported trigger), and beyond that just that vasodilators generally can be expected to trigger an attack when in cycle. Maybe keep the part "The role of diet and specific foods in triggering cluster headaches is controversial and not well understood." Right now, it sounds like a bunch of edits from people that got headaches after eating sushi, so they added "and sushi too!" Greghodg ( talk) 17:49, 4 August 2010 (UTC)
Deep brain stimulation
Why is there no mention of deep brain stimulation on this page? Take a look at this link: http://www.bbc.co.uk/blogs/thereporters/ferguswalsh/2010/12/brain_surgery_to_relieve_headaches.html Reissgo ( talk) 08:34, 18 December 2010 (UTC)
LSD
===Low-dose psychedelics===
There is anecdotal evidence that serotonergic psychedelics such as psilocybin (mushrooms), LSD, and LSA ( d-Lysergic acid amide, contained by Rivea corymbosa seeds) abort cluster periods and extend remission periods. The doses needed to affect cluster headaches start below those needed to produce psychedelic effects. [1] [2] [3] Melatonin, psilocybin, serotonin, and the triptan abortive drugs are closely-related tryptamines.
Researchers at McLean Hospital/Harvard Medical School investigated the ability of psilocybin ("magic mushrooms") and LSD to treat cluster headaches through medical record review and interview of 53 patients who had used either/both drug, reporting in Neurology that the majority described partial or complete relief from cluster attacks. [4] A clinical study of these treatments under the auspices of Clusterbusters is the next intended phase of research at McLean Hospital, Harvard Medical School. [5] [6]
This needs to be based on review articles per WP:MEDRS Doc James ( talk · contribs · email) 13:21, 19 January 2011 (UTC)
- Here's one: Sun-Edelstein C, Mauskop A. (2011). "Alternative headache treatments: nutraceuticals, behavioral and physical treatments". Headache: the Journal of Head and Face Pain. 51 (3): 469–83. doi: 10.1111/j.1526-4610.2011.01846.x. PMID 21352222. Sasata ( talk) 05:22, 17 November 2011 (UTC)
Infobox image
At the moment, Clusterhead.jpg is the image in the infobox, visible at the very top of the page. While this image may be useful later in the article, I am of the opinion that as far as lead images go, this is actually worse than having no image at all. Quickly jumping from the article title to this image will lead the reader to believe that the article is about a piece of art, and certainly not a medical condition. I welcome arguments or suggestions, but if no one objects, I may just swap out the image myself. -- Cryptic C62 · Talk 04:39, 17 November 2011 (UTC)
- It's now been removed. — Hex (❝?!❞) 11:55, 5 November 2012 (UTC)
"Atypical Facial Pain Syndrome"
This comment has been hidden, as
Wikipedia does not provide medical advice.
|
|---|
| Wikipedia does not provide medical advice. The following comment seeks medical advice. This is not a suitable place. Please seek a real-life medical professional. Comments from well-meaning Wikipedians may not represent best practice in the poster's country of origin, and there is a danger that best practice may be misrepresented or, at worst, deliberately distorted. No further edits should be made to this discussion. |
|
I was sent to an ONT who said I had "Atypical Facial Pain Syndrome". When I said "that doesn't really say anything other than what I just described to you" he said "it's also known as cluster migraines." Is this generally accepted? I ask because I see no reference to it here. -- Richardson mcphillips ( talk) 19:48, 14 March 2012 (UTC)
|
2012 review in the BMJ
[2] Doc James ( talk · contribs · email) 08:15, 15 April 2012 (UTC)
Copyright
Copyright violating content is illegal and cannot be allowed in the articles. However, the following citation may be useful:
causa sui ( talk) 18:33, 19 May 2013 (UTC)
- A) The text you removed was the following sentence:
- Although controversial, case reports suggest that ingesting psilocybin or LSD can reduce cluster headache pain and interrupt cluster headache cycles.
- The abstract, located
here, contains the following sentence:
- Although controversial, there are some reports demonstrating the benefit of recreational drugs such as marijuana, lysergic acid diethylamide and psilocybin in headache treatment.
- With the exception of the initial two words, "Although controversial", the two sentences are almost completely different. Your robust assertion of a "copyright violation" is baffling, when simply removing those two words would have done. See WP:LIMITED.
- B) You clearly didn't bother to read the diff before blindly hitting revert, as I had fixed the problem while undoing your strange deletion. The text in my version read:
- Some case reports have also suggested that ingesting LSD, psilocybin or cannabis can reduce cluster headache pain and interrupt cluster headache cycles.
- Consequently I have now restored it. — Scott • talk 22:38, 19 May 2013 (UTC)
Psilocybin and LSD
As a casual reader, this section strikes me as odd, for this line: "For many sufferers, the legal risks pale in comparison to the pain caused by the condition.[citation needed]", specifically the need for the citation? As the article has already established several times that people are willing to commit suicide to end the pain, and those are cited. So I feel that there's no need for a source - it's just reasonable to assume that any legal problems would not be as big of a deal to plenty of people who are suicidal. — Preceding unsigned comment added by 50.124.52.204 ( talk) 04:57, 1 June 2013 (UTC)
- The source is necessary because conclusions drawn by the writer are agains WP:NOR PinkShinyRose ( talk) 20:58, 28 July 2013 (UTC)
Bias: introduction of the "Management" section, third paragraph
Except for the first sentence this paragraph is only relevant to the US. I think the first sentence should remain (maybe rephrased to fit into a prior paragraph), but the remaining part of the paragraph should be separate and start out by explicitly stating that it is relevant only to the US (maybe by starting the paragraph by "In the US there are difficulties in treatment arising from the recent pressure of the DEA. Depending on the state...". Should the first sentence be rephrased or just appended to the previous paragraph? Does anyone disagree about clarifying the limited scope of the paragraph in the first sentence? PinkShinyRose ( talk) 21:08, 28 July 2013 (UTC)
merger proposal: Cluster headache treatments
I don't see anything especially notable in the other page that isnt already here, and I don't see the point of this redundancy. It also tends to be a spam/NPOV attractor. -- [ UseTheCommandLine ~/ talk ]# ▄ 17:59, 28 August 2013 (UTC)
- I didn't know that existed. It should definitely be merged here. — Scott • talk 22:09, 28 August 2013 (UTC)
I have completed the merge. This page needs additional attention and I would be happy to collaboratively edit if there are any interested editors. LT90001 ( talk) 03:05, 12 October 2013 (UTC)
Cleanup
- Edit: I refer to this edit, removing my cleanup tags.
I have marked this page for cleanup because it uses numerous primary sources, has excessive use of dated, experimental or primary sources, with conflicting advice; and requires general copy-editing. This is not a comment on a particular source or treatment methodology, just that this article needs some work overall. Kind regards, LT910001 ( talk) 04:18, 13 October 2013 (UTC)
| This is an archive of past discussions. Do not edit the contents of this page. If you wish to start a new discussion or revive an old one, please do so on the current talk page. |
| Archive 1 |
- ^ "Hallucinogenic Treatment of Neuro-Vascular Headaches". ClusterBusters. Retrieved 2006-09-22.
- ^ Mark Honigsbaum (2005-08-02). "Headache sufferers flout new drug law - Calls for clinical trials and rethink of legislation as patients claim that magic mushrooms can relieve excruciating condition". The Guardian. Retrieved 2006-09-22. [reprint by Multidisciplinary Association for Psychedelic Studies]
- ^ Arran Frood (2008-10-07). "LSD cured my headache - Cluster headaches cause such severe pain that some sufferers are driven to suicide. Now one man believes he's found a surprising cure". The Independent. Retrieved 2008-10-07.
-
^ Sewell R, Halpern J, Pope H (2006).
"Response of cluster headache to psilocybin and LSD" (
PDF). Neurology. 66 (12): 1920–2.
doi:
10.1212/01.wnl.0000219761.05466.43.
PMID
16801660.
{{ cite journal}}: Unknown parameter|month=ignored ( help)CS1 maint: multiple names: authors list ( link) - a Brief Communications, also presented as:
Sewell, R. Andrew, M.D.; Halpern, John M., M.D. "The Effects Of Psilocybin And LSD On Cluster Headache: A Series Of 53 Cases." Abstract. Presented to the National Headache Foundation’s Annual Headache Research Summit. February, 2006. Twenty-two of 26 psilocybin users reported that psilocybin aborted attacks; 25 of 48 psilocybin users and 7 of 8 LSD users reported cluster period termination; 18 of 19 psilocybin users and 4 of 5 LSD users reported remission period extension. - ^ "Research into psilocybin and LSD as potential treatments for people with cluster headaches". LSD and Psilocybin Research. Multidisciplinary Association for Psychedelic Studies. Retrieved 2006-09-22.
- ^ "Response of Cluster Headache to Psilocybin and LSD" Chapter 5 in "Psychedelic Medicine: New Evidence for Hallucinogens as Treatment" Michael Winkelman and Thomas B. Roberts (editors) (2007) Westport, CT: Praeger/Greenwood.