This article may be too technical for most readers to understand. (August 2016) |
| Accessory auricle | |
|---|---|
 | |
| Specialty | Dermatology |
An accessory auricle is a congenital anomaly typically seen as a skin coloured nodule, most frequently just to the front of the ear. [1] [2]
Signs and symptoms

The general presentation is of a skin-covered nodule, papule, or nodule of the skin surface, usually immediately anterior to the auricle. [2] However, it may be anywhere within the periauricular tissues. [2] Bilateral presentation can be seen. [2]
Genetics
A study of a family with 11 affected showed the accessory auricle were inherited in an autosomal dominant manner. [3]
Diagnosis
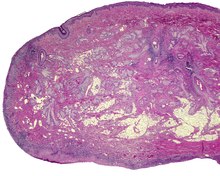
The lesions presents as a nodule or papule, either sessile or pedunculated. They may be soft or have a cartilaginous structure. By histologic examination, it is a recapitulation of normal external auricle. There will be skin, cartilaginous structures, and cartilage (although the later is not seen in all variants of this disorder). [4] [5] Some investigators believe that the tragus is the only hillock which is derived from the first branchial arch. This is clearly suggestive that true cases of Accessory Auricle represent a true duplication of the hillocks that were part of the second branchial arch. [6] The second ear appears as a mirror image folded forward and lying on the posterior cheek.[ citation needed]
Differential diagnosis
These structures are distinctly different from squamous papilloma and benign teratoma.[ citation needed]
Classification
The several components or degrees of development range from an ear tag, preauricular appendage, preauricular tag, or accessory tragus, to supernumerary ears or polyotia. [7] It is a relatively common congenital anomaly of the first branchial arch or second branchial arches. Other anomalies may be present concurrently, including cleft palate, cleft lip, or mandibular hypoplasia. There is a known association with Goldenhar syndrome (oculo-auriculo-vertebral syndrome) [8] and with Wildervanck syndrome. [9] [10] [11] There may also be an association with congenital cartilaginous rest of the neck.[ citation needed]
Management
Simple surgical excision is curative. [12] The recommended treatment is that the skin is peeled off the extra-auricular tissue and protruding cartilage remnants are trimmed. [13] Normal appearance is achieved in majority of cases. The reconstruction successful in true cases of accessory auricle, as it also is in individuals with auricular appendages. [14] [15]
Epidemiology
These lesions usually present in neonates, although they may not come to clinical attention until adulthood (for cosmetic reasons). There is no gender predilection. They are present in approximately 3-6 per 1000 live births. [16]
References
- ^ Hwang, Jungil; Cho, Jaeyoung; Burm, Jin Sik (September 2018). "Accessory auricle: Classification according to location, protrusion pattern and body shape". Archives of Plastic Surgery. 45 (5): 411–417. doi: 10.5999/aps.2018.00430. PMC 6177632. PMID 30282411.
- ^ a b c d Cardesa, Antonio (2016). "8. Ear and temporal bone". In Franchi, Alessandro; Slootweg, Pieter J.; Gale, Nina; Ann, Sandison (eds.). Pathology of the Head and Neck. Springer. p. 397. ISBN 978-3-662-49670-1.
- ^ Yang, Y; et al. (2006). "A locus for autosomal dominant accessory auricular anomaly maps to 14q11.2–q12". Human Genetics. 120 (1): 144–147. doi: 10.1007/s00439-006-0206-1. PMID 16775710. S2CID 1196716.
- ^ Jansen, T.; Romiti, R.; Altmeyer, P. (2000). "Accessory tragus: Report of two cases and review of the literature". Pediatric Dermatology. 17 (5): 391–394. doi: 10.1046/j.1525-1470.2000.017005391.x. PMID 11085670. S2CID 19325370.
- ^ Brownstein, M. H.; Wanger, N.; Helwig, E. B. (1971). "Accessory tragi". Archives of Dermatology. 104 (6): 625–631. doi: 10.1001/archderm.1971.04000240049006. PMID 5131708.
- ^ Stevenson, Roger E.; Hall, Judith G. (2005). Human Malformations and Related Anomalies (2nd ed.). Oxford University Press. pp. 339–340. ISBN 978-0199748082.
- ^ Lam, J.; Dohil, M. (2007). "Multiple Accessory Tragi and Hemifacial Microsomia". Pediatric Dermatology. 24 (6): 657–658. doi: 10.1111/j.1525-1470.2007.00560.x. PMID 18035991. S2CID 19272462.
- ^ Konaş, E.; Canter, H. I.; Mavili, M. E. (2006). "Goldenhar complex with atypical associated anomalies: Is the spectrum still widening?". Journal of Craniofacial Surgery. 17 (4): 669–672. doi: 10.1097/00001665-200607000-00011. PMID 16877912.
- ^ Tadini, G.; Cambiaghi, S.; Scarabelli, G.; Brusasco, A.; Vigo, P. (1993). "Familial occurrence of isolated accessory tragi". Pediatric Dermatology. 10 (1): 26–28. doi: 10.1111/j.1525-1470.1993.tb00006.x. PMID 8493161. S2CID 20872067.
- ^ Gao, J. Z.; Chen, Y. M.; Gao, Y. P. (1990). "A survey of accessory auricle anomaly. Pedigree analysis of seven cases". Archives of Otolaryngology–Head & Neck Surgery. 116 (10): 1194–1196. doi: 10.1001/archotol.1990.01870100088019. PMID 2206506.
- ^ Resnick, K. I.; Soltani, K.; Bernstein, J. E.; Fathizadeh, A. (1981). "Accessory tragi and associated syndromes involving the first branchial arch". The Journal of Dermatologic Surgery and Oncology. 7 (1): 39–41. doi: 10.1111/j.1524-4725.1981.tb00591.x. PMID 7204730.
- ^ Pan, B.; Qie, S.; Zhao, Y.; Tang, X.; Lin, L.; Yang, Q.; Zhuang, H.; Jiang, H. (2010). "Surgical management of polyotia". Journal of Plastic, Reconstructive & Aesthetic Surgery. 63 (8): 1283–1288. doi: 10.1016/j.bjps.2009.06.037. PMID 19617017.
- ^ Scott-Brown's Otorhinolaryngology (7th ed.). Hodder Arnold. 2016-06-15. p. 969. ISBN 978-0-340-808-931.
- ^ Ku, PK; Tong, MC; Yue, V (1998). "Polyotia- a rare external ear anomaly". International Journal of Pediatric Otorhinolaryngology. 46 (1–2): 117–20. doi: 10.1016/S0165-5876(98)00152-9. PMID 10190712.
- ^ Bendor-Samuel, RL; Tung, TC; Chen, YR (1995). "Polyotia". Annals of Plastic Surgery. 34 (6): 650–2. doi: 10.1097/00000637-199506000-00015. PMID 7661545. S2CID 220587660.
- ^ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. p. 894. ISBN 978-1-4160-2999-1.
Further reading
- Lester D. R. Thompson; Bruce M. Wenig (2011). Diagnostic Pathology: Head and Neck. Hagerstown, MD: Lippincott Williams & Wilkins. pp. 7:2–3. ISBN 978-1-931884-61-7.
External links
This article may be too technical for most readers to understand. (August 2016) |
| Accessory auricle | |
|---|---|
|
| |
| Specialty | Dermatology |
An accessory auricle is a congenital anomaly typically seen as a skin coloured nodule, most frequently just to the front of the ear. [1] [2]
Signs and symptoms
The general presentation is of a skin-covered nodule, papule, or nodule of the skin surface, usually immediately anterior to the auricle. [2] However, it may be anywhere within the periauricular tissues. [2] Bilateral presentation can be seen. [2]
Genetics
A study of a family with 11 affected showed the accessory auricle were inherited in an autosomal dominant manner. [3]
Diagnosis
The lesions presents as a nodule or papule, either sessile or pedunculated. They may be soft or have a cartilaginous structure. By histologic examination, it is a recapitulation of normal external auricle. There will be skin, cartilaginous structures, and cartilage (although the later is not seen in all variants of this disorder). [4] [5] Some investigators believe that the tragus is the only hillock which is derived from the first branchial arch. This is clearly suggestive that true cases of Accessory Auricle represent a true duplication of the hillocks that were part of the second branchial arch. [6] The second ear appears as a mirror image folded forward and lying on the posterior cheek.[ citation needed]
Differential diagnosis
These structures are distinctly different from squamous papilloma and benign teratoma.[ citation needed]
Classification
The several components or degrees of development range from an ear tag, preauricular appendage, preauricular tag, or accessory tragus, to supernumerary ears or polyotia. [7] It is a relatively common congenital anomaly of the first branchial arch or second branchial arches. Other anomalies may be present concurrently, including cleft palate, cleft lip, or mandibular hypoplasia. There is a known association with Goldenhar syndrome (oculo-auriculo-vertebral syndrome) [8] and with Wildervanck syndrome. [9] [10] [11] There may also be an association with congenital cartilaginous rest of the neck.[ citation needed]
Management
Simple surgical excision is curative. [12] The recommended treatment is that the skin is peeled off the extra-auricular tissue and protruding cartilage remnants are trimmed. [13] Normal appearance is achieved in majority of cases. The reconstruction successful in true cases of accessory auricle, as it also is in individuals with auricular appendages. [14] [15]
Epidemiology
These lesions usually present in neonates, although they may not come to clinical attention until adulthood (for cosmetic reasons). There is no gender predilection. They are present in approximately 3-6 per 1000 live births. [16]
References
- ^ Hwang, Jungil; Cho, Jaeyoung; Burm, Jin Sik (September 2018). "Accessory auricle: Classification according to location, protrusion pattern and body shape". Archives of Plastic Surgery. 45 (5): 411–417. doi: 10.5999/aps.2018.00430. PMC 6177632. PMID 30282411.
- ^ a b c d Cardesa, Antonio (2016). "8. Ear and temporal bone". In Franchi, Alessandro; Slootweg, Pieter J.; Gale, Nina; Ann, Sandison (eds.). Pathology of the Head and Neck. Springer. p. 397. ISBN 978-3-662-49670-1.
- ^ Yang, Y; et al. (2006). "A locus for autosomal dominant accessory auricular anomaly maps to 14q11.2–q12". Human Genetics. 120 (1): 144–147. doi: 10.1007/s00439-006-0206-1. PMID 16775710. S2CID 1196716.
- ^ Jansen, T.; Romiti, R.; Altmeyer, P. (2000). "Accessory tragus: Report of two cases and review of the literature". Pediatric Dermatology. 17 (5): 391–394. doi: 10.1046/j.1525-1470.2000.017005391.x. PMID 11085670. S2CID 19325370.
- ^ Brownstein, M. H.; Wanger, N.; Helwig, E. B. (1971). "Accessory tragi". Archives of Dermatology. 104 (6): 625–631. doi: 10.1001/archderm.1971.04000240049006. PMID 5131708.
- ^ Stevenson, Roger E.; Hall, Judith G. (2005). Human Malformations and Related Anomalies (2nd ed.). Oxford University Press. pp. 339–340. ISBN 978-0199748082.
- ^ Lam, J.; Dohil, M. (2007). "Multiple Accessory Tragi and Hemifacial Microsomia". Pediatric Dermatology. 24 (6): 657–658. doi: 10.1111/j.1525-1470.2007.00560.x. PMID 18035991. S2CID 19272462.
- ^ Konaş, E.; Canter, H. I.; Mavili, M. E. (2006). "Goldenhar complex with atypical associated anomalies: Is the spectrum still widening?". Journal of Craniofacial Surgery. 17 (4): 669–672. doi: 10.1097/00001665-200607000-00011. PMID 16877912.
- ^ Tadini, G.; Cambiaghi, S.; Scarabelli, G.; Brusasco, A.; Vigo, P. (1993). "Familial occurrence of isolated accessory tragi". Pediatric Dermatology. 10 (1): 26–28. doi: 10.1111/j.1525-1470.1993.tb00006.x. PMID 8493161. S2CID 20872067.
- ^ Gao, J. Z.; Chen, Y. M.; Gao, Y. P. (1990). "A survey of accessory auricle anomaly. Pedigree analysis of seven cases". Archives of Otolaryngology–Head & Neck Surgery. 116 (10): 1194–1196. doi: 10.1001/archotol.1990.01870100088019. PMID 2206506.
- ^ Resnick, K. I.; Soltani, K.; Bernstein, J. E.; Fathizadeh, A. (1981). "Accessory tragi and associated syndromes involving the first branchial arch". The Journal of Dermatologic Surgery and Oncology. 7 (1): 39–41. doi: 10.1111/j.1524-4725.1981.tb00591.x. PMID 7204730.
- ^ Pan, B.; Qie, S.; Zhao, Y.; Tang, X.; Lin, L.; Yang, Q.; Zhuang, H.; Jiang, H. (2010). "Surgical management of polyotia". Journal of Plastic, Reconstructive & Aesthetic Surgery. 63 (8): 1283–1288. doi: 10.1016/j.bjps.2009.06.037. PMID 19617017.
- ^ Scott-Brown's Otorhinolaryngology (7th ed.). Hodder Arnold. 2016-06-15. p. 969. ISBN 978-0-340-808-931.
- ^ Ku, PK; Tong, MC; Yue, V (1998). "Polyotia- a rare external ear anomaly". International Journal of Pediatric Otorhinolaryngology. 46 (1–2): 117–20. doi: 10.1016/S0165-5876(98)00152-9. PMID 10190712.
- ^ Bendor-Samuel, RL; Tung, TC; Chen, YR (1995). "Polyotia". Annals of Plastic Surgery. 34 (6): 650–2. doi: 10.1097/00000637-199506000-00015. PMID 7661545. S2CID 220587660.
- ^ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. p. 894. ISBN 978-1-4160-2999-1.
Further reading
- Lester D. R. Thompson; Bruce M. Wenig (2011). Diagnostic Pathology: Head and Neck. Hagerstown, MD: Lippincott Williams & Wilkins. pp. 7:2–3. ISBN 978-1-931884-61-7.